| 8 |
Statistical observations on acute ‘radiation’ sickness in Hiroshima and Nagasaki |
The standard narrative of the atomic bombings implies that a)all those exposed near the hypocenter with light or no shielding received lethal doses of radiation, b)those exposed at 2 km or more from the hypocenter should have been safe from acute radiation sickness (ARS), and c)radiation intensities high enough to cause ARS prevailed only for a few seconds during the detonations themselves. This story fails to account for the following observations:
- there is a substantial number of survivors who were exposed near the hypocenter, either in the open or protected only by wooden houses;
- there are victims of ARS at distances which should have been safe;
- in Hiroshima, multiple cases of ARS, some with lethal outcome, were recorded among those who were not in the city during the bombing but entered it shortly afterwards;
- in survivors, a history of ARS correlates very poorly with official radiation dose estimates; one third of the survivors in the highest dose group did not report even a single characteristic symptom of ARS.
The observed distribution of ARS in time and space thus clearly contradicts the claimed causation by radiation released in a single strong pulse.
| 8.1 |
Physical assumptions |
Before delving into the data themselves, we will note some assumptions which concern physical conditions and methods, and which will guide the interpretation of the medical data.
| 8.1.1 |
Radiation doses from fallout and induced radioactivity are negligible |
As discussed earlier (Section 2.5), the most important forms of radiation from a fission bomb are the γ-rays and neutrons released during the blast itself. In contrast, residual radioactivity on the ground due to fallout and to neutron capture should be minor; while it might pose some health risk in those exposed to it for long periods of time, residual radioactivity should not cause or contribute to acute radiation sickness. Cullings et al. [30] put it succinctly:
The radiation doses were truly acute, being received almost completely in a matter of seconds; furthermore, every person in each city received the dose at the same time … The situation regarding residual radiation was most recently reviewed in the DS86 Final Report.94 As that report makes clear, doses from residual radiation are generally believed to be small.
Note that the authors arrived at this conclusion when starting from orthodox tenets regarding the inner workings and the explosive yields of the nuclear bombs. Thus, we don’t need to assume that no nuclear detonations ever happened in order to dismiss fallout and neutron-induced radiation as possible causes of ARS; we are not making a circular argument.95
| 8.1.2 |
Biology trumps physics in the detection of lethal radiation |
All physical dosimeters and radiation counters are subject to measurement errors; but no frayed cable, leaky battery, or distracted operator can prevent the lethal effect of radiation on a human being.
The lethal dose of radiation for humans is approximately 8 Sv; with γ-radiation, this is the same as 8 Gy.96 The only possible way to survive such a dose is through a bone marrow transplant, which of course was not available to the bombing victims. Indeed, total body irradiation with a lethal dose of γ-rays is one of two methods used to condition leukemia patients for a bone marrow transplant. Once a patient receives some 10 Gy of γ-rays as a single dose, his bone marrow will die—as will, hopefully, all of his leukemic cells, for that is the real purpose of the procedure; and so will he, unless transplanted with the bone marrow of a healthy donor immediately afterwards. Irradiation could not serve this purpose if it were anything but deadly every single time.
If a human being does not die, it did not receive a lethal dose; there can be no false-negative reading. Thus, if a physical measurement or calculation indicates that lethal radiation prevailed at a certain time and place, but a human who was present then and there survived, then this biological outcome categorically falsifies the physical statement.
False-positive findings of sickness and death due to radiation can, of course, be produced with ‘radiomimetic’ compounds such as sulfur mustard; and accordingly the second conditioning method for bone marrow transplant is the use of drugs exactly of this kind.97
| 8.2 |
Manifestations of acute radiation sickness |
The seriousness of acute radiation sickness depends, above all, on the dose of the radiation received. Other important considerations are whether that dose is delivered all at once or in multiple sessions, and whether it is applied to the whole body or only to some part of it. In a nuclear detonation, irradiation should usually affect the whole body evenly, and accordingly all doses stated in the following should be taken as whole-body doses.98 Also important are type and particle energy of the radiation; this is discussed in Section 2.9.2.
The sensitivity to radiation differs greatly between tissues and cell types in the body, and therefore different organs will respond at different threshold doses. Three sub-syndromes that concern different target organs can be distinguished.
| 8.2.1 |
The hematopoetic syndrome |
This syndrome is caused by damage to bone marrow stem cells, which are among the most radiosensitive cell types.99 It becomes manifest at doses above 1.5-2 Sv, and no patients who received more than 5-6 Sv will survive it if intensive medical care is unavailable. All types of blood cells are descended from bone marrow stem cells, and thus all of them will fail to be renewed in hematopoetic syndrome (HS for short). However, the consequences are most dramatic with the white blood cells and with thrombocytes, since these are short-lived (see Figure 8.4). In contrast, mature red blood cells have a life span of 120 days; they can sustain the patient even when their regeneration ceases for several weeks, and they will thus not limit his lifespan in the acute phase of HS.
When leukocytes fail, the patients will suffer from infections; when platelets are depleted, bleeding will occur spontaneously or after minor trauma. Numerous scattered hemorrhagic spots will arise which are most readily observed beneath the skin or the mucous membranes of the oral cavity, but which equally affect the inner organs; and in severe cases, the patient may bleed to death internally. This condition is referred to as purpura, and the characteristic hemorrhagic spots are called petechiae.
As long as some bone marrow stem cells survive, blood cell formation will eventually resume; if levels of white blood cells and of platelets fall dangerously low, they may be transiently substituted by transfusion. If all stem cells were wiped out, then only a transplant of bone marrow from a compatible donor can possibly save the patient.
Radiation doses similar to those that damage the bone marrow will also damage the hair follicles. In this case, too, loss of function may be transient or permanent; higher doses will cause greater loss of hair, and permanent hair loss may occur at doses similar to those that irreversibly destroy the bone marrow. Thus, hair loss provides a useful proxy for estimating the extent of damage to the bone marrow.
| 8.2.2 |
The gastrointestinal syndrome |
At doses of 6 Sv and above, damage to the intestines will give rise to diarrhea and often outright intestinal bleeding. The breakdown of the gut barrier will facilitate infections, which will be made worse by the depletion of white blood cells. Loss of fluid and electrolytes will further aggravate the situation. Intensive care with antibiotics and replacement of fluids and electrolytes, in addition to treatment of the hematopoetic syndrome, may rescue patients with doses up to 10-12 Sv, but at dosages higher than this the prognosis of gastrointestinal syndrome becomes hopeless. Of course, none of these therapeutic measures were available in Hiroshima and Nagasaki; under those conditions, practically all patients with manifest gastrointestinal syndrome should have died.
| 8.2.3 |
The cerebrovascular syndrome |
At very high doses—the threshold doses given in the literature vary considerably, reflecting the paucity of clearly documented cases; but a widely cited IAEA report states 20 Gy [149]—radiation will kill within 1-2 days by direct action on the central nervous system. It is believed that damage primarily affects the small blood vessels in the brain; inhibited perfusion then causes various manifestations of brain dysfunction, most conspicuously coma.
Hall and Giaccia [150, p. 218] point out that, even though neurological symptoms may initially dominate the clinical picture, the damage to the vascular system is likely general. This matches their case descriptions of two workers who developed cerebrovascular syndrome after receiving extremely high doses of irradiation by accident, and who also suffered general circulatory shock, to which they succumbed within two days after the exposure.
| 8.2.4 |
Prodromal and latent stages |
The hematopoetic and gastrointestinal syndromes described above take days or weeks to become fully manifest; and, for reasons explained in Section 2.11, the delay will be longer with lower radiation doses. Minutes to hours after exposure, however, there will be some early signs, less severe and less characteristic. Most common at this prodromal stage are vomiting and mild headache; diarrhea and fever indicate higher doses and presage later manifestation of gastrointestinal syndrome. In all but the most severe cases, these prodromal signs subside, and the patients will enter a latent stage showing few clinical symptoms or none at all. During this time, however, cell proliferation within the bone marrow and, at higher doses, within the intestine drops off, and the specific syndromes manifest themselves once the initially surviving maturing or fully mature cells in these organs expire.
| 8.3 |
Acute radiation doses in Hiroshima and Nagasaki |
The tenet that, in Hiroshima and Nagasaki, doses sufficient to cause acute radiation sickness could have been inflicted only during the blast itself (see Section 8.1.1) gives rise to a number of testable predictions, which we will examine in the following.
| 8.3.1 |
Radiation dose as a function of distance from the hypocenter |
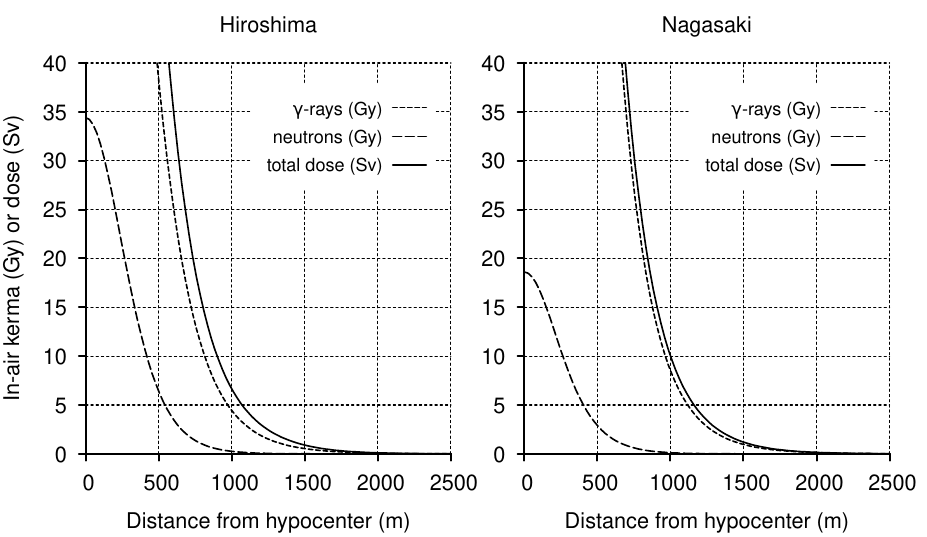
Since there were no instruments in place to measure the radiation doses when the detonations occurred, we have to make do with approximations based on indirect methods and calculations. The officially endorsed dose estimates have seen some fairly considerable changes over time. Figure 8.1 depicts the biologically effective or equivalent doses for both Hiroshima and Nagasaki, based on current estimates of γ-ray and neutron intensities [30]. In this graph, the biological dose was calculated by applying an experimentally determined dose-dependent relative biological efficiency (RBE) function for neutron radiation [48] to the neutron component of Cullings’ radiation levels.
| 8.3.2 |
Shielding from radiation by buildings |
The dose estimates in Figure 8.1 apply to persons who were directly in the path of the radiation, without any sort of solid matter between them and the point of the detonation up in the air (the epicenter). However, many people were indoors at the time of the bombing, and some of those who found themselves outdoors were shaded from the detonation by some intervening structure.
Traditional Japanese houses were simple buildings with one or two stories, constructed mainly from wood, sometimes with thatched roofs but usually with tiled ones. This was the predominant type of building in both Hiroshima and in Nagasaki, although in the latter city the proportion of concrete buildings is said to have been somewhat higher. The penetration of γ-rays and fast neutrons into such traditionally constructed buildings was studied quite thoroughly in the 1950s and 60s, as documented by Arakawa [151], and Auxier [36]. According to these measurements, γ-ray doses inside such buildings would have been ≥ 60%, and neutron doses ≥ 40% of those in the open. Thus, these buildings would have given only very limited protection from bomb radiation. In contrast, buildings constructed from concrete could have provided effective shielding, particularly within rooms facing away from the detonation.
| 8.3.3 |
Threshold distances for radiation doses |
Considering the almost complete lack of medical care available to the bombing victims, we can assume that survival of more than 6 Sv would have been impossible; according to the estimate shown in Figure 8.1, this threshold is reached or exceeded in both cities at distances up to 1000 m. Accordingly, there should have been no possibility of surviving an unshielded exposure within 1000 m in either Hiroshima or Nagasaki. Within 500 m, unshielded doses should invariably have caused cerebrovascular syndrome, the most severe and rapidly deadly form of ARS; and this should apply not only to persons without shielding, but also to those shielded by no more than a traditional wooden house. On the other hand, beyond 1500 m in both cities, the unshielded dose drops to a level below which no serious manifestations of acute radiation sickness are to be expected.
| 8.3.4 |
Predicted distance distribution of ARS |
From the foregoing observations, we can conclude that the statistics on ARS in Hiroshima and Nagasaki should exhibit a highly regular pattern, with the following characteristics:
- within 500 m, all of those exposed without shielding or inside traditional wooden houses should have suffered cerebrovascular syndrome, and none of them should have survived beyond 2-3 days;
- between 0.5 and 1 km, ARS should have occurred in all persons exposed inside wooden houses or without shielding; and in the latter group, there should be no survivors;
- between 1 km and 1.5 km, a very large proportion of victims who were exposed with light shielding or in the open should have suffered ARS, ranging from mild and transient to violent and deadly;
- at most a few light cases of ARS should have occurred among those exposed beyond 1.5 km, regardless of shielding;
- absolutely no ARS cases whatsoever should have occurred beyond a distance of 2 km.
Note that these threshold distance values are based on current dose estimates. Early estimates were substantially higher [151,152]. If we assume that those earlier numbers were in fact correct, then a similar pattern should still emerge, but with each of the boundaries stated in the list above approximately 500 m further out.
| 8.4 |
Observed distance distribution of ARS in Hiroshima |
We will now compare observed occurrences of ARS and of survival to predicted ones. The two key sources for this purpose are Oughterson et al. [33] and Sutou [34]. Both studies report statistics on several thousand individuals. The first one was compiled by the ‘Joint Commission for the Investigation of the Effects of the Atomic Bomb in Japan’, a group of American and Japanese physicians convened at the initiative of Ashley W. Oughterson, a professor of surgery at Yale who at the time was serving as a colonel in the U.S. military. This commission only arrived at Hiroshima and Nagasaki in October 1945, but it did acquire and organize data previously collected by Japanese physicians; and the statistical evaluation of these earlier Japanese data constitutes the main substance of the commission’s report. Most of the figures tabulated in [33] pertain to patients still alive and in medical care at 20 days after the bombings; recorded are slightly below 7000 survivors in each of the two cities.100
The second study was carried out in 1957 by Dr. Gensaku Oho,101 a physician from Hiroshima, who enlisted the help of student volunteers to canvas the resident population of Hiroshima. The main purpose of this study was to determine the occurrence of radiation sickness among persons who had not been exposed to the bombings themselves, but who had entered the area close to the hypocenter only afterwards. The more recent paper by Sutou [34], which is used here, is a partial translation of and commentary on Oho’s earlier study.
| 8.4.1 |
Survival of persons exposed within 500 m of the hypocenter |
The first prediction is that no one should have survived beyond a few days who was exposed, with light shielding or without it, within 500 m of the hypocenter. This prediction is falsified by the following findings:
- Twelve of Oho’s respondents in 1957 reported having been exposed within 0.5 km of the hypocenter. Of these, one had been exposed outdoors, whereas eleven had been indoors; presumably, at least some among this number had been inside wooden buildings.
- Keller [10] lists eight patients at Osaka University Hospital as having been exposed inside wooden buildings within no more than 500 m, and among them four had been within 50 m. He further states that of all patients in his survey five succumbed, and that the average day of death among these five was 26 days after the bombing. Therefore, at least three patients exposed within 500 m the hypocenter were still alive some four weeks after the bombing. Even the patients who did succumb within four weeks had survived long enough to be transported to Osaka, and therefore must have lived longer than compatible with cerebrovascular syndrome, which they invariably should have suffered.
This number of confirmed survivors is certainly very small, which means that the inferno in the city center must have been every bit as deadly as eyewitness testimony indicates [14,156] (see also Figure 8.2). Nevertheless, if we accept that there are any survivors at all, then this finding alone disproves the story of the nuclear detonation, and no amount of physical studies can possibly salvage it—remember that no false-negative measurements are possible with our Homo sapiens reference dosimeter.
| 8.4.2 |
Survival and incidence of ARS among patients exposed within 1 km of the hypocenter |
| Outdoors, unshielded | Inside Japanese building | |||||
| Distance (km) | Alive at 20 d | E/P (%) | † | Alive at 20 d | E/P (%) | † |
| 0–1.0 | 105 | 88.6 | 22 | 410 | 85.9 | 120 |
| 1.1–1.5 | 249 | 42.6 | 9 | 560 | 38.6 | 19 |
| 1.6–2.0 | 689 | 14.2 | 4 | 754 | 10.1 | 3 |
| 2.1–2.5 | 590 | 6.8 | 1 | 731 | 4.7 | 0 |
| 2.6–3.0 | 192 | 7.8 | 0 | 390 | 2.6 | 0 |
| 3.1–4.0 | 159 | 3.8 | 0 | 325 | 1.2 | 0 |
| 4.1–5.0 | 68 | 2.9 | 0 | 127 | 0.8 | 0 |
Oughterson et al. [33] do not separate exposure within 0.5 km from that within 1 km, presumably because they considered the numbers in the former group too low. However, beginning with 1 km, they group patients by distance intervals of 0.5 km, and they carefully subdivide each group according to different types of shielding. Table 8.1 contains a selection of these data, on which we can make the following observations:
-
On the twentieth day, 88.6% of patients exposed within 1 km and in the open
have developed specific symptoms of radiation sickness, which means that 11.4% have
not. Similar proportions are found with those who were exposed while inside Japanese
style houses.
With doses as high as those predicted for this range, the latency period of ARS should last at most 8-18 days [31]. Therefore, the observation of patients who on the 20th day still show no signs of manifest ARS deviates from expectation.
-
Of the 105 patients exposed in the open and still alive on the 20th day,
only 22 are known to have died later on. Oughterson et al. [33] quite sensibly
state:
It is probable that other unreported deaths occurred in this group of people, and some may have died as a result of radiation after the end of the survey in Japan.
However, they also show (in their Table 58) that death rates steadily declined as time went on. Out of a total of 6663 patients recorded in Hiroshima as being alive on the 20th day, 254 or 4% are reported to have died subsequently. 137 of these deaths occurred between days 20 and 29, whereas only two occurred between days 70 and 79, and another five occurred between day 80 and the unspecified end date of the survey. Considering this time course, it is highly likely that most of the 83 patients who had been exposed in the open within 1 km, and who had survived the entire time period of the study, also remained alive thereafter—in marked contrast to the expectation that they should all have perished.102
In summary, while the proportion of ARS sufferers in this group is large, it is not as large as predicted. Even more difficult to explain is the number of those who experienced ARS yet survived it.
| 8.4.3 |
Incidence of ARS at >1 km from the hypocenter |
Above, we stated that a large proportion of persons within 1-1.5 km should suffer from ARS. In patients exposed without shielding or with light shielding only, the proportion listed in Table 8.1 is close to 40%. While this is low, we must allow that in some cases the symptoms may not yet have been manifest on the survey’s reference date, for at dosages below 4 Gy the latency period may exceed 20 days [31]. In contrast, the mortality is again implausibly low. The ARS cases observed beyond 2 km from the hypocenter—at frequencies below 10% and decreasing with distance, but not quite dropping to zero even between 4 and 5 km—differ from expectation unequivocally; they are not explained even by the highest published estimates of acute radiation doses.
The above findings were confirmed by Oho, who documented cases of ARS among survivors who had been at ≥ 2 and even ≥ 3 km from the hypocenter during the detonation. Importantly, this applied even to some survivors who had stayed away from the hypocenter for several weeks after the bombing [34].
| 8.5 |
Observed distance distribution of ARS in Nagasaki |
The observations made above for Hiroshima mostly apply to Nagasaki as well (see Table 68N in [33]); however, some findings are quantitatively more pronounced. Symptoms of and death due to ARS are less frequent within 1 km than in Hiroshima, even though radiation doses are supposed to have been higher (see Figure 8.1): among survivors exposed in the open or shielded only by a wooden house, less than 60% exhibit epilation or purpura. Among survivors exposed between 1.5-2.5 km, a greater percentage than at Hiroshima shows symptoms of ARS. On the other hand, beyond 4 km from the hypocenter, that percentage does indeed drop to zero in Nagasaki, whereas it remains positive even at this distance in Hiroshima.
| 8.6 |
ARS symptoms in people shielded by concrete buildings |
Concrete buildings will afford substantial protection from both γ-rays and neutron radiation, and we should therefore expect a lower number of ARS victims among those inside these buildings than in those inside wooden buildings or in the open. This is indeed observed; within 1 km from the hypocenter, the incidence of ARS is approximately 25% lower inside heavy buildings than outside, both in Hiroshima and Nagasaki (Oughterson et al. [33], Tables 68H and 68N). Yet, ARS inside heavy buildings in Hiroshima remains more prevalent than it is in the open in Nagasaki, even though the radiation dose is said to have been higher in Nagasaki.
| Layer effecting 90% attenuation (cm) | ||
| Material | γ-rays | fast neutrons |
| Iron | 9-13 | |
| Concrete | 30-45 | 26-28 |
| Wood | 125-175 | |
| Water | 65-92 | |
| Soil | 45-65 | |
More detailed statistics on this question are reported by Oughterson and Warren [146], who in their Table 3.7 show findings from three individual concrete buildings in Hiroshima, all of which were situated between 700 and 900 meters from the hypocenter. In each building, some people were protected by multiple walls or floors, such that the total shielding was equivalent to ≥ 154 inches (or 394 cm) of water (see Table 8.2). The stated radiation dose outside the buildings was up to 80 Gy, which amounts to approximately ten times the lethal dose. However, after passing through this much shielding, it should have been attenuated to a mere 4 mGy. This corresponds to just 2/3 of the typical annual dose of a U.S. citizen and will, of course, not produce any acute symptoms at all.
Nevertheless, Oughterson and Warren report cases of ARS—some of them lethal—among persons thus protected. They propose that these may be due to neutrons, apparently assuming that neutrons are less effectively shielded by concrete than are γ-rays. However, this is now known to be incorrect (see Table 8.2); and moreover, as already noted, the estimated neutron dose at Hiroshima was very substantially reduced in the decades after their book was published [49].
As a second deus ex machina, the authors suggest that the bomb’s γ-radiation may have been of much higher particle energy, and therefore more penetrating, than is generally assumed. However, they do not offer a physical basis for this hypothesis, nor do they pursue its wider implications for the physical and medical dosimetry of the entire event, which would have been substantial. Such lack of thoroughness suggests that the authors themselves do not take their own proposal seriously. When commenting on the reverse scenario—the wondrous survival of some individuals exposed to strong γ-radiation—the authors dispense with any special pleading and blankly state (p. 63):
It is equally difficult to explain the complete absence of radiation effects in a number of people who were theoretically exposed to lethal dosages of radiation.
We note that Oughterson and Warren acknowledge the dilemma of ARS occurring among those beyond the reach of the bomb’s radiation, while failing to appear in some of those exposed to a ‘theoretically lethal’ dose. Adjusting dose estimates will not solve this dilemma: increasing doses may avoid the Scylla of death despite protection, but it will wreck the ship on the Charybdis of inexplicable survival; assuming lower doses to explain miraculous survival will make the deaths of shielded victims all the more incomprehensible.
| 8.7 |
ARS in people who were outside Hiroshima at the time of the bombing |
The occurrence of ARS symptoms in persons who were outside Hiroshima on the day of the bombing, but who entered the zone within 1 km of the hypocenter afterwards, is a crucial piece of evidence. While anecdotal reports are found in many sources [12,14,16,32,62], the only statistical survey on this question is the one by Gensaku Oho; and it is telling that we owe this crucial study to the personal initiative of this energetic doctor from Hiroshima and his student volunteers, rather than to the official institutions created and maintained for such investigations by the governments of the United States and of Japan.
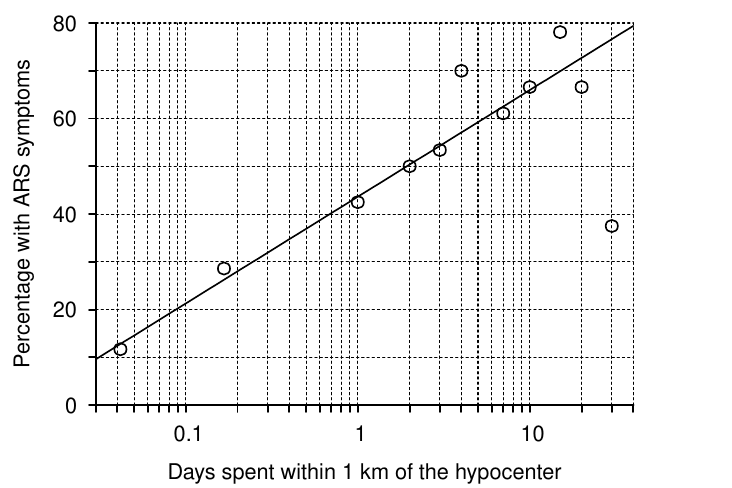
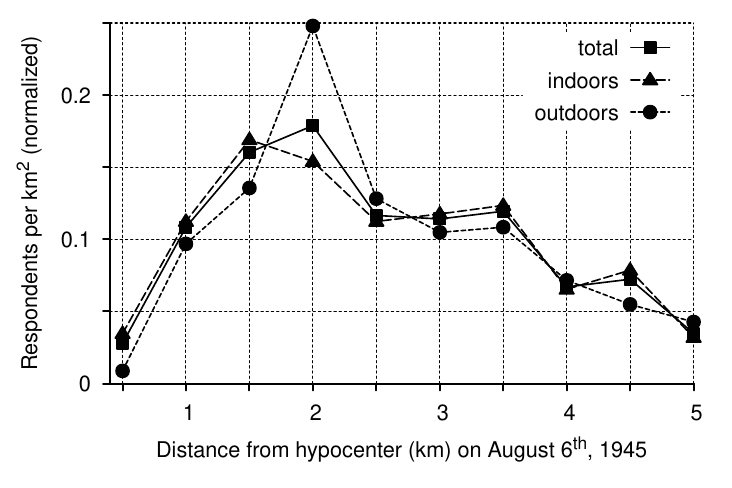
Oho’s most important findings are summarized in Figure 8.3. Many people entering the area within 1 km of the hypocenter report symptoms of ARS; the percentage of people thus affected exceeds 50% among those who stayed for more than 2 days. Additional tables and figures presented by Sutou [34] clearly document that the same effect is also present among those who were in Hiroshima during the bombing: while of course many in this group suffered ARS regardless of their whereabouts in the aftermath, the incidence is higher among those who also came near the hypocenter in that period.103
Findings such as those reported by Oho can, of course, not be explained with the radiation released during the detonation. There are three ways of dealing with this problem:
- The findings are ascribed to fallout or residual radiation, which are assumed to have been much greater than conventional or official estimates [34,158,159].
- The findings are declared to ‘warrant further analysis’ and then studiously ignored [36, p. 90].
- The findings are ignored without ceremony. If you guessed that this is the most common approach, you are indeed correct.
The last two alternatives require no further comment. Regarding the first one, it was shown earlier that real fallout must have been lower, not higher than the official estimates, and there is no basis whatsoever for higher estimates of neutron-induced radioactivity.104
The thesis of this book—namely, that sulfur mustard, not radiation was the cause of ‘ARS’—provides a ready explanation for cases of the disease among late entrants to the city. Sulfur mustard is known to linger, and its persistent stench was noted by Burchett four weeks after the bombing [16]. Wind-driven mustard fumes would explain why those located downwind from the hypocenter suffered more ARS [158] and were at greater risk of developing cancer [160,161]. While Yamada and Jones [158] ascribe the surplus incidence of ARS in this group to high β-radiation from isotopes contained in the black rain, the very low levels of 137Cs in extant black rain samples [6] clearly disprove their explanation.105
| 8.8 |
Late-onset ARS |
In patients who suffered ARS due to exposure only after the bombing, the symptoms should develop with some delay; and this is indeed reflected in the statistics reported by Oughterson et al. [33].
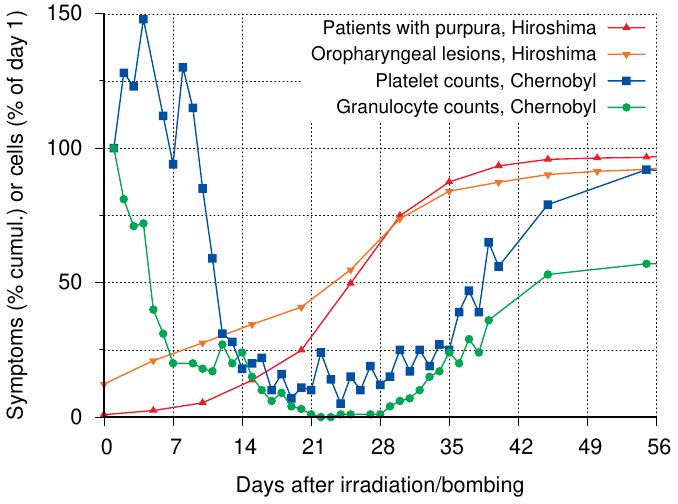
Characteristic symptoms of ARS hematopoetic syndrome (see Section 8.2.1) are purpura, caused by the failure of the blood platelets, and oropharyngeal ulcers due to bacterial and fungal infections, which are brought on by the lack of granulocytes. In patients who exhibit these symptoms after exposure to a single dose of irradiation, they become manifest between days 8 and 28, with shorter latency at higher doses [149]. Figure 8.4 shows that this is also true of most Hiroshima bombing victims; however, in about 25%, the initial manifestation is delayed until the fifth week or later.106 For illustration, the figure also shows the time course of platelet and granulocyte counts in patients exposed to irradiation after the reactor meltdown at Chernobyl. Both cell counts reach their lowest point before the 28th day, which explains that symptoms will be manifest by this time.
Anecdotal evidence confirms the occurrence of late cases. For example, in his posthumously107 published book First into Nagasaki [166], the American journalist George Weller notes on September 22nd:
New cases of atomic bomb poisoning with an approximate fifty percent death rate are still appearing at Nagasaki’s hospital six weeks after the blow fell … Whereas formerly twenty patients a day with dwindling hair and their bone marrow affected were coming to Japanese hospitals, the rate is now fallen to about ten.
The decreasing, yet still ongoing observation of new cases agrees with the data in Figure 8.4. While from this limited information we cannot be sure whether the death rate in new cases was indeed falling, this would be plausible in real ARS [149] and similarly also in mustard gas poisoning. What is not plausible in true ARS, however, is the repeated occurrence of new cases, particularly ones with fatal outcome, as late as six weeks after the exposure. These patients must have taken in the poison some time after the bombings, probably in a cumulative fashion, just like some of the subjects surveyed by Oho [34].108
| 8.9 |
ARS symptoms and official radiation dose estimates |
You may have seen studies on atomic bomb survivors that correlate some biological outcome such as cancer with individual radiation doses. The question of dosimetry will be discussed in Chapter 11, which also shows a graph which correlates the incidence of ARS symptoms radiation doses (Figure 11.1B). The correlation is obviously very poor, and the dose-response curve is wildly implausible biologically, as can be seen by comparison with proper data shown in Figure 11.1A.
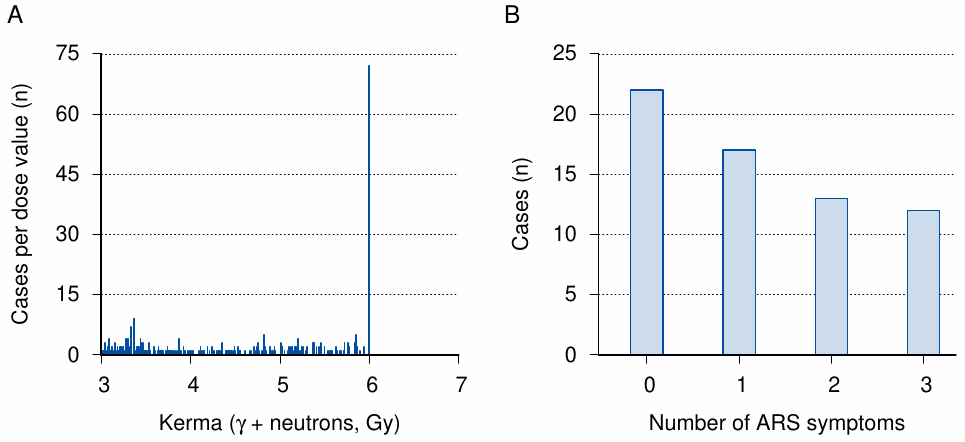
The data set from which Figure 11.1B was constructed contains radiation doses at higher resolution than depicted in the figure. If we plot a histogram of the number of people grouped by the individual dose values in the file, we see that the dataset contains no cases with estimated doses above 6 Gy (Figure 8.5 A). However, the number of people with an assigned dose of exactly 6.000 Gy greatly exceeds that of any other individual dose value above 3 Gy; in fact, only below 1 Gy do we find dose values with higher head counts than 6 Gy exactly. This peculiar pattern strongly suggests that all raw dose estimates higher than 6 Gy were simply truncated at that value; probably because they were deemed unsurvivable, and quite possibly under the impression of the rhesus monkey experiments shown in Figure 11.1A. It should go without saying that such sausage-making does not qualify as science. Furthermore, whether truncated or not, in this highest of all dose groups, the number of individuals with 0 or only one symptom of ARS exceeds that with two or more symptoms (Figure 8.5B). The 22 individuals without any symptoms clearly count among Warren’s and Oughterson’s mystery patients with ‘complete absence of radiation effects’ in spite of exposure to ‘theoretically lethal’ doses of radiation.
The findings presented in this section reinforce our previous observation that the distribution of ARS does not fit the official story of the bomb and its radiation. We will revisit the question of purported radiation doses and biological effects in Chapters 11 and 12.
| 8.10 |
Diarrhea as an early symptom of ARS |
Before leaving this topic, one recurrent motif in the reports on ‘radiation sickness’ from Hiroshima and Nagasaki should be noted: the widespread and early occurrence of diarrhea, often bloody, among the patients. A graphic account is given by Michihiko Hachiya [62]. The author, a head physician who had been injured in the bombing and admitted as a patient to his own hospital, wrote in his diary on August 7th:
Everything was in disorder. And to make matters worse was the vomiting and diarrhea. Patients who could not walk urinated and defecated where they lay. Those who could walk would feel their way to the exits and relieve themselves there. Persons entering or leaving the hospital could not avoid stepping in the filth, so closely was it spread. The front entrance became covered with feces overnight, and nothing could be done for there were no bed pans and, even if there had been, no one to carry them to the patients.
Disposing of the dead was a minor problem, but to clean the rooms and corridors of urine, feces, and vomitus was impossible.
Such events would suggest an outbreak of some virulent enteric pathogen, which is indeed common in disaster situations; and Hachiya and his staff initially assumed this to be the case. Also on August 7th, Hachiya writes:
Dr. Hanaoka … brought word that there were many who not only had diarrhea but bloody stools and that some had had as many as forty to fifty stools during the previous night.109 This convinced me that we were dealing with bacillary dysentery and had no choice but to isolate those who were infected.
Dr. Koyama, as deputy director, was given the responsibility of setting up an isolation ward.
However, already on August 13th, he notes:
My conjecture that deaths were due to the effects of a germ bomb causing dysentery I had to discard because diarrhea and bloody stools were decreasing.
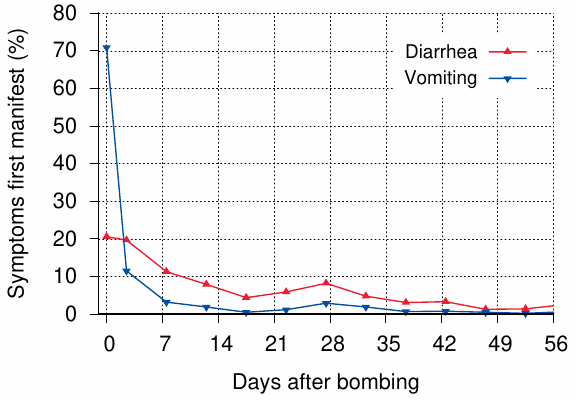
Hachiya’s conclusions are confirmed by the data given in Oughterson et al. [33], which show that both bloody and non-bloody diarrhea are strongly correlated with other ARS symptoms, and also that case numbers were highest early on and then declined (Figure 8.6), even though the hygienic conditions remained about as bad as can be imagined.
Diarrhea can indeed occur in real radiation sickness. However, it commonly occurs very early on only in patients who have received a dose of 6 Sv or greater [149]. Under the conditions then prevailing in Hiroshima and Nagasaki, patients hit with such a high dose would not have survived. Yet, the data listed by Oughterson et al. [33] pertain to patients who were alive 20 days after the bombing, and 96% of whom remained alive when the study concluded several months later (see Section 8.4.2), which means that they were not lethally irradiated. Thus, the timing of diarrhea observed in Hiroshima also indicates that the reported radiation sickness was not actually caused by radiation. On the other hand, early onset diarrhea has been described in multiple reports on mustard gas exposure of humans and of experimental animals (see Section 7.3.5).
| 8.11 |
The curse of the pharaohs |
Many of the data presented in this chapter were drawn from the report of the Joint Commission [33], and we saw that these data contain clear evidence against nuclear detonations as the cause of ARS in Hiroshima and Nagasaki. We thus might wonder what the commission’s members, most of whom were physicians, were really thinking while they assembled their data. The only first-hand account by any of them which I have found is that by the pathologist Averill Liebow [77]. The author offers many interesting glimpses into the conditions of the work, but he does not betray any doubt or puzzlement concerning its scientific findings. However, writing originally in 1965, Liebow notes:
It is true that few who took part are left to tell … Indeed it is as though some curse, like that which the superstitious say fell upon Lord Carnarvon and his men when they violated the tomb of Pharaoh Tut-ankh-amen, has been visited upon those who pried into the ravaged heart of Hiroshima. Only three of the seven American medical officers live. Drs. Oughterson and Tsuzuki, the chief organizers for the two countries, have died; so too, while still young, have Drs. Calvin Koch, Jack D. Rosenbaum, and Milton R. Kramer. May this record do honor to these able and devoted men.
Liebow’s analogy surely is intriguing. We will, however, leave it for others to pursue, lest we be accused of superstition.