| 10 |
Early clinical and pathological findings in the bombing victims |
In this chapter, we will scrutinize both eyewitness testimony and the medical literature in order to understand the symptoms observed in the bombing victims immediately or shortly after the event. Key observations include:
- early fatalities suffered acute lung damage, sometimes with secondary effects such as ocular compartment syndrome. These manifestations are compatible with mustard gas inhalation, but they have not been reported in accidental cases of extremely high and rapidly fatal irradiation;
- the medical literature on the bombing victims reports not a single case of acute retinal burns, which should have been common among those who reported having looked a the ‘nuclear flash’;
- pathological reports on internal organs in early fatalities, while scarce, nevertheless point to mustard gas rather than radiation as the underlying cause.
Overall, these findings reinforce the conclusions reached in the preceding chapters on acute radiation sickness and on skin burns.
Chapter 8 discussed the acute medical effects of the bombings from a quantitative, statistical point of view. In this chapter, we will look at them in more qualitative detail. The evidence available for this purpose is limited. In the hours and days following the bombings, chaos reigned, and none of those who died during this time received adequate diagnosis and treatment. Their sufferings and symptoms are described only in the scattered testimony of eyewitnesses, both laypersons and medical doctors, who were anguished as much by the apocalyptic scenes around them as by their inability to help.122
Important sources for this chapter include the recollections by two Japanese physicians. We already mentioned the diary by Michihiko Hachiya [62] from Hiroshima, a detailed account by an experienced, perceptive, and compassionate observer; this document should be read by anyone interested in the humanitarian dimension of the disaster. From Nagasaki, there is the report by Tatsuichiro Akizuki [167], a more junior physician, who unlike Hachiya was not himself incapacitated in the attack123 and therefore was able to give more detailed observations on the victims immediately after the bombing.124 The reports by Oughterson and colleagues [33,146] will again be used. The one by Oughterson and Warren [146] includes a chapter by Liebow et al. on the autopsy material collected mostly by Japanese pathologists, which was published independently as a journal article elsewhere [42].
In addition to the above books and reports, which were all written by physicians or medical scientists, important detail can be found in eyewitness accounts by non-specialists. The compilations of such testimony by [14] and by Sekimori [156] are particularly valuable.
| 10.1 |
Clinical picture in early fatalities |
| 10.1.1 |
Symptoms apparent immediately after the bombing |
On the day of the Nagasaki bombing, Dr. Tatsuichiro Akizuki was on duty at his hospital in the Urakami district, 1800 m from the hypocenter. The building was damaged and partly destroyed by fire, but all of the staff and the patients quickly escaped and initially survived.
The attack had occurred at 11 a.m.; shortly afterwards, the first victims from outside began to arrive, seeking help:
About ten minutes after the explosion, a big man, half-naked, holding his head between his hands, came into the yard towards me … ‘Got hurt, sir,’ he groaned; he shivered as if he were cold. ‘I’m hurt.’
I stared at him, at the strange-looking man. Then I saw it was Mr. Zenjiro Tsujiomoto, a market gardener and a friendly neighbor to me and the hospital. I wondered what had happened to the robust Zenjiro. ‘What’s the matter with you, Tsujimoto?’ I asked him, holding him in my arms.
‘In the pumpkin field over there—getting pumpkins for the patients—got hurt…’ he said, speaking brokenly and breathing feebly. It was all he could do to keep standing. Yet it didn’t occur to me that he had been seriously injured.
‘Come along now,’ I said, ‘You are perfectly all right. I assure you. Where’s your shirt? Lie down and rest somewhere where it’s cool. I’ll be with you in a moment.’
His head and his face were whitish; his hair was singed. It was because his eyelashes had been scorched away that he seemed so bleary-eyed. He was half-naked because his shirt had been burned from his back in a single flash. …
Another person who looked just like him wandered into the yard. … ‘Help me,’ he said, groaning, half-naked, holding his head between his hands. He sat down, exhausted. ‘Water … Water …’ he whispered.
As time passed, more and more people in similar plight came up to the hospital—ten minutes, twenty minutes, an hour after the explosion. All were of the same appearance, sounded the same. ‘I’m hurt, hurt! I’m burning! Water!’ … Half-naked or stark naked, they walked with strange, slow steps, groaning from deep inside themselves … they looked whitish. … One victim who managed to reach the hospital asked ‘Is this a hospital?’ before suddenly collapsing on the ground. …
‘Water, water’ they cried. They went instinctively down to the banks of the stream [below the hospital], because their bodies had been scorched and their throats were parched and inflamed; they were thirsty. I didn’t realize then that these were the symptoms of ‘flash burn.’
Thus far, Akizuki has described victims whom he had encountered within one hour or so of the attack. At this early stage, we can make the following observations:
- Akizuki does not immediately recognize his ‘strange-looking’ neighbor, which suggests that his features are already somewhat distorted. They will be much more so later in the day.
- He notices some signs of immediate burns—singed hair and eyelashes, as well as nudity (see Section 9.4).
- Akizuki does not describe any other outward signs of injury; instead, he reassures his suffering neighbor that he is alright.
- The victims speak hoarsely; their throats are ‘parched and inflamed,’ and they are thirsty; their breath is labored.
- The victims are pale and weak, and some collapse.
- The victims are holding their heads between their hands, suggesting that they have a severe headache.
| 10.1.2 |
Symptoms apparent after several hours |
While the above observations capture the early stage of the injuries, the victims’ aspect is strikingly transformed later on. Here is Akizuki’s description:
In the afternoon a change was noticeable in the appearance of the injured people who came up to the hospital. The crowd of ghosts which had looked whitish in the morning were now burned black. Their hair was burnt; their skin, which was charred and blackened, blistered and peeled. Such were those who now came toiling up to the hospital yard and fell there weakly.
These victims might have come from another district of the city, further away from the hospital but closer to the hypocenter, where they might have suffered more severe immediate burns. However, a similar change is also apparent in the victims who had arrived earlier. While on his way to help an injured colleague, he again encounters some of them:
When I reached the little river, I came across an astonishing scene. Half-naked or nearly naked people were crouching at the water’s edge. All looked alike, without distinction of sex or age; long hair was the only clue to the female sex. On one side their bodies had been grilled and were highly inflamed. The procession of white ghosts which had passed me some time before had gathered here on the bank of the stream, seeking water to relieve the terrible thirst and the scorching pain of their bodies. Crowds of these victims lined the stream.
‘Oh, how it hurts! I’m hurting—burning!’ said Mr. Tsujimoto, groaning. His face, which had been whitish, when I saw him earlier, was now darker, blackened; his lips were swollen. His wife sat not far away, her face and body also blackened, moaning insensibly.
It is clear that, in this group of patients at least, overt symptoms have become manifest with a delay of several hours. They are now obvious even in the wife of Mr. Tsujimoto, whom Akizuki had not even mentioned as being afflicted earlier on.125 Still later in the day, Akizuki describes both Mr. and Mrs. Tsujimoto as ‘cinder-burnt.’ While Mrs. Tsujiomoto will live for a few more days, her husband expires the same night:
At about midnight, Mr Tsujimoto’s condition suddenly worsened. … By degrees, Mr. Tsujimoto’s breathing became harsher. I couldn’t feel any pulse. … Suddenly Mr. Tsujimoto went into a violent fit of convulsions; his eyes bulged. ‘His last moment has come!’ said someone.
Labored breathing in the bombing victims is confirmed by another eyewitness from Nagasaki, Akira Nagasaka [156, p. 74]:
A woman, probably in her mid-thirties, was lying on the ground, her hair wild, her clothes in tatters, her face red with blood. She was putting all the strength that remained in her to raise her head and murmur, “Water, water.”
When I had gathered my wits about me, I scooped some dirty water out of a nearby ditch and gave it to her. She drank it as if it were the most delicious thing ever to pass her lips, but most of it merely trickled down her chin onto her breast. “More, please,” she begged, but she could do no more than gasp for breath when I brought it, having no strength left to drink.
The testimony from Hiroshima is, if anything, even more gruesome.126 Eyewitness Kosaku Okabe [156, p. 35] was not near the hypocenter for the bombing, but he came upon the scene in downtown Hiroshima several hours afterwards:
Wherever a puddle of water had collected from burst water pipes, people had gathered like ants around a honey pot. Many had died where they lay at the water’s edge, their strength gone. Others had clambered over the dead bodies to get at the water, only to die in the same way, their bodies piling one on top of another.
Okabe also describes the aspect of the victims:
Most people had been wearing light summer shirts that morning. But most of the dead were bare chested, and many were completely naked, perhaps because their clothes had been burned off them. The parts of the body that had been exposed to the flash had suffered great burns, and the skin was turning purple and trailing from the body in strips.
In every case, the eyeballs of the dead were either protruding from their sockets or hanging out completely. Blood had gushed from the mouth, ears, and nose. The tongue had swelled to the size of a golf ball and had pushed its way out of the mouth, gripped tightly by the teeth. The whole anatomy seemed to have been destroyed. Most bodies were bloated, and it was often impossible to tell whether they were male or female.
The grisly, apocalyptic picture painted by Okabe’s testimony might seem exaggerated, but each detail is confirmed by other eyewitnesses [14,156,180]. While the victims described by Okabe are already dead, another witness depicts the scene when some of them are still alive. Hachiya [62] relates the observations told him on August 6th by one of his visitors, Mr. Hashimoto, who was already mentioned in the preceding chapter. Like Okabe, Hashimoto entered the inner city after the bombing:
When I reached the Misasa railway bridge … I encountered a dead man. I saw many others in the water tanks fighting for breath. The sight was horrible.
Mr. Hashimoto also describes the days following the bombing:
During those days, wherever you went, there were so many dead lying around it was impossible to walk without encountering them—swollen, discolored bodies with froth oozing from their noses and mouths.
Overall, the testimony given by several independent witnesses from the two cities is remarkably consistent. We therefore can’t dismiss it, but instead must try to understand what exactly could have caused such terrible injury and disfigurement.
| 10.1.3 |
Pathophysiological interpretation of early symptoms |
Before identifying the causes, we must take a step back and consider what the clinical signs observed in these victims tell us about the underlying pathophysiology.
| 10.1.3.1 |
Skin burns |
A key observation here is that in some victims at least, such as the Tsujimotos, burns of the skin were manifest only after some hours, as is typical with mustard gas. The blackened aspect of the skin in such cases was most likely caused by intense cyanosis rather than ‘scorching,’ which should have been apparent immediately (see for example Figure 9.5C). It is quite likely, of course, that some victims suffered both immediate (napalm) and delayed burns.
| 10.1.3.2 |
Circulatory shock and capillary leak syndrome |
The initial paleness reported by Akizuki in patients who arrived on foot at his clinic suggests beginning circulatory shock. At a more advanced stage of shock, paleness may give way to cyanosis; this is observed by Akizuki in some of the initially pale patients at a later time, and it is also described by Okabe in the victims that he encounters several hours after the Hiroshima bombing.
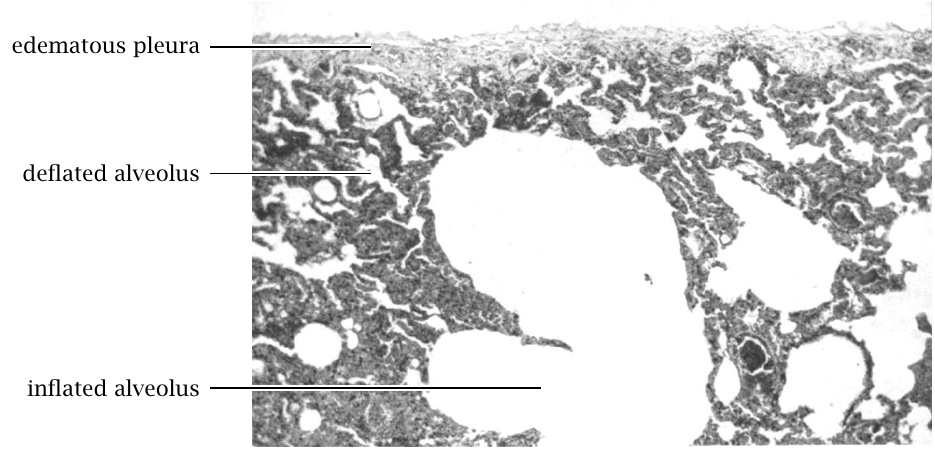
Shock may be accompanied by capillary leak syndrome, which causes intense thirst and, after intake of large volumes of water, extreme edema (Figure 10.1). All of these symptoms were described in the bombing victims.
A related observation is the acute headache, which is suggested by Akizuki’s description of patients holding their heads between their hands. Headaches are caused by vascular distension in the meninges; the simultaneous occurrence with shock suggest that the latter was likely caused in part by the loss of vascular tone.

| 10.1.3.3 |
Injury to the lungs and airways |
Acute respiratory distress is described in early fatalities, but both Hachiya and Akizuki also report labored breathing in the patients they examine in the subsequent days and weeks. Immediate affliction of the upper airways can be surmised from Akizuki’s observation of hoarseness in the victims he meets shortly after the bombing.
The froth oozing from mouths and noses noted by the sharp-eyed Mr. Hashimoto in the dead bombing victims indicates severe pulmonary edema, while outright bleeding from the mouth and nose, described by Okabe, suggests injury to blood vessels in the mucous membranes of the airways, and possibly to larger vessels inside the chest.
Also pertinent is Dr. Masao Tsuzuki’s remark on the ‘suffocating pain’ experienced by those who inhaled the gas which ‘permeated immediately after the explosion of the atomic bomb’ (see Section 1.4.4). Overall, it is plain that some noxious agent released at Hiroshima and Nagasaki attacked the lungs and airways.
| 10.1.3.4 |
Traumatic asphyxia and orbital compartment syndrome |
With the assumptions of capillary leak syndrome and injury to the lungs and airways, we can account for the thirst, the general edema, the respiratory distress, the cyanosis, as well as the blood and froth spilling from the mouth and nose. The peeling skin is, at this point of the exposition, no longer a mystery. That leaves the bleeding from the ears and the eyeballs protruding or even hanging out. How can we fit these into the picture?
The protruding eyeballs are a telltale sign of orbital compartment syndrome. The eye socket (Latin: orbita) is a confined space, and if some irregular process such as edema or hemorrhage claims some of that space, then the eyeball is displaced outwards. One contributing factor would have been the capillary leak syndrome, but there most likely was another one—traumatic asphyxia, also known as Perthes syndrome. Most commonly, traumatic asphyxia is triggered by compression of the thorax, but it can also occur with other causes of disrupted respiration, including severe asthma attacks [182]. It arises when pressure to the chest or injury to the lungs prevents blood pumped by the right heart from entering the lungs. The blood therefore backs up into the right heart and from there into the large veins that supply it, particularly those within the head. Blood vessels become distended, the blood stagnating within them becomes desaturated of oxygen, its color turning dark, and plasma fluid leaks into the tissues; the patient’s face turns purple and swollen. Bursting blood vessels may cause bleeding from all cranial orifices, including the ears. Bleeding could likewise have occurred behind the eyeballs; in fact, the convulsions and bulging eyeballs in the dying Mr. Tsujimoto suggest some such event. Since severe lung damage was present in the bombing victims, we can conclude that the preconditions for traumatic asphyxia were met.
While traumatic asphyxia and ocular compartment syndrome are both rare in normal life, there is indeed at least one clinical case report that describes them in combination [183]. As it turns out, the severely injured patient in this case also developed capillary leak syndrome. The authors state that capillary leakage preceded the orbital compartment syndrome, and they consider it a contributing cause of the latter.
Based on the foregoing, it stands to reason that the combination of lung and vascular injury present in the bombing victims could also account for the development of orbital compartment syndrome.127 We can thus reduce the overall clinical picture to three fundamental pathophysiological effects:
- injury to the lungs and airways;
- injury to the vasculature, leading to capillary leak syndrome and shock;
- injury to the skin, causing it to peel.
| 10.1.4 |
Causal attribution |
What could have caused these three effects? The easy part of the answer is that neither ‘flash burn’ nor ionizing radiation can account for this entire clinical picture. As discussed in Section 9.6, flash burns should have been visible in some form immediately, but Akizuki fails to notice them in several patients whom he encounters shortly after the bombing. Without very severe exterior burns, there simply is no mechanism by which a flash of light could produce acute respiratory distress.
As regards ionizing radiation, here is the case description of a patient who received approximately five times a lethal dose of it [150, p. 218]:
In a nuclear criticality accident at Los Alamos in 1958, one worker received a total body dose of mixed neutron and γ-radiation estimated to be between 39 and 49 Gy. Parts of his body may have received as much as 120 Gy. This person went into a state of shock immediately and was unconscious within a few minutes. After 8 hours, no lymphocytes were found in the circulating blood, and there was virtually a complete urinary shutdown despite the administration of large amounts of fluids. The patient died 35 hours after the accident.
This patient received a dose of radiation about as high as it could have been near the hypocenter in Hiroshima. He promptly developed cerebrovascular syndrome and also general circulatory shock, and he quickly died of it—without intensive care, he probably would have died on the same day, as did many of the victims in Hiroshima and Nagasaki. However, no mention is made of facial or general cyanosis, respiratory distress, peeling skin, or dangling eyes. Since he lost consciousness so quickly, he would not have had time enough to find a puddle and drink enough water to swell up to any great extent. Thus, apart from shock and rapid death, his clinical picture bears no resemblance to that described in the victims at Hiroshima and Nagasaki.
Animal experiments reported by Bloom et al. [26] showed the lungs to have relatively low susceptibility to radiation; lethal whole-body doses of X-rays or neutrons produced little or no evidence of lung tissue damage when compared to controls.128 The skin, too, showed very minor effects at such doses. While these findings do of course not rule out lung or skin damage with supra-lethal irradiation, they exclude preferential damage to these organs, which is evident in the Hiroshima and Nagasaki victims.
The more difficult and interesting part of the answer concerns how we actually can account for the clinical picture. Since we already have evidence that napalm and mustard gas were used, we will examine if they can explain it.
| 10.1.4.1 |
Napalm |
Mr. Tsujimoto, the patient most thoroughly described by Akizuki (Section 10.1.1), has lost his shirt in the bombing, and his hair and eyelashes are singed. Even though he does not present any obvious burns at the time, this does suggest some possible exposure to napalm, albeit probably not through a major direct hit.
According to Björnerstedt et al. [141], the fire from a sufficiently large napalm bomb will inflict harm through radiating heat even at some distance. Moreover, conventional burns can cause smoke inhalation injury, which can result in acute respiratory distress with rapid deadly outcome [185]. Severe burns will also cause circulatory shock; and with napalm, this may occur even when only some 10% of the total body surface have been burned [143]. Thus, napalm could in principle set off the pathophysiological cascade that would produce all of the symptoms seen in the early fatalities, and this may well have happened in some of them.
It is doubtful, however, that napalm was the only cause in Mr. Tsujimoto’s case. Smoke inhalation injury tends to occur with fires indoors, since here the smoke accumulates in a confined space; Mr. Tsujimoto, however, reported having been hurt while harvesting pumpkins in the field. Conceivably, one might also suffer smoke inhalation injury outdoors, if surrounded and trapped by fire; but it seems unlikely that one could escape such an inferno without also receiving significant burns to the skin. According to Dolinin [143], asphyxia occurs in approximately 5% of napalm victims, particularly in those with manifest burns to the face. Overall, napalm seems unlikely as the cause of respiratory distress in Mr. Tsujimoto, or in the other victims with similar early symptoms. We thus should consider the possible role of mustard gas.
| 10.1.4.2 |
Mustard gas |
I should note upfront that the literature does not report any clinical cases of mustard gas poisoning which exhibit the complete picture described in Section 10.1.2. While capillary leak syndrome and extensive damage to the skin and lungs are documented (see Chapter 7), I have not found a single case report on traumatic asphyxia caused by mustard gas. Nevertheless, I propose that exactly this did occur at Hiroshima and Nagasaki. My reason is that the bombing victims must have sustained much graver acute lung injury than any earlier victims—their sufferings, even though caused by poison gas, were indeed ‘worse than poison gas’. In World War I, mustard gas was introduced only after other poison gases had been, so that the soldiers who encountered it were already equipped with gas masks. Likewise, gas masks had also been worn by the poisoned mustard gas factory workers described by Warthin and Weller [109]. In contrast, the victims at Hiroshima and Nagasaki had no warning and no protection, and they must have inhaled the gas in far greater amounts than those earlier victims.
As a consequence of such high doses to the lungs, the airways would have become clogged by swelling mucous membranes, fibrin plugs, and blood clots (see Section 7.3.2). Air becoming trapped behind such obstacles—acute emphysema—would have raised the pressure inside the chest and compressed the pulmonary veins, thus preventing the flow of blood returning from the body and the head. Additionally, clots would have formed within the lungs’ blood vessels themselves, further impeding the flow of blood back into the lungs. In the most severely poisoned victims, the acute obstruction of the airways and the lung circulation would have been incomparably worse than in any asthma attack.129
Pulmonary effects similar to those just described for mustard gas have also been documented for smoke inhalation injury [187], which is common in napalm burn victims.
| 10.1.4.3 |
Possible use of other lung poisons |
While in my estimation mustard gas can account for the acute lung toxicity which occurred among early fatalities, the use of other lung poisons cannot be ruled out. Both chlorine and phosgene were used in World War 1 and caused acute and severe lung damage among their victims [109,139]. Another plausible candidate is lewisite, which is known to have been produced and tested by the U.S. during World War II [21], and whose acute effects resemble those of sulfur mustard but arise more rapidly, probably due to its greater volatility [35].
Our final, somewhat surprising candidate is cadmium. Apart from napalm, the Americans also employed a second incendiary in their firebombing raids, namely magnesium-thermate bombs. One variant of this bomb type, the AN-M50TA2, contained a ‘secret toxic agent’ [188, p. 429] which was later identified as cadmium [189].130 The high temperature produced by the burning thermate and magnesium should vaporize the cadmium. The medical literature reports several cases of acute lung toxicity due to inhalation of cadmium vapors, sometimes fatal [190,191]. A reference text on drugs and poisons [192, p. 1767] notes diarrhea among the symptoms of acute poisoning; as noted in Section 8.10, acute diarrhea was common also among the bombing victims. Thus, if AN-M50TA2 bombs were indeed used, then it stands to reason that vaporized cadmium released from them would have contributed to acute toxicity among the victims. However, as will be discussed in Section 13.2.5, I have not found any clear indications that this weapon was indeed employed in the ‘nuclear’ bombings.
Chapter 7 already explained why lewisite is unlikely to have been used instead of mustard gas rather than in addition to it. The reasons given there apply to the other poisons discussed in this section also.
| 10.1.5 |
Conclusion |
In summary, therefore, I propose that napalm and mustard gas, alone or in combination, can account for the full clinical picture observed in the early fatalities, while radiation cannot. Mustard gas was very likely the dominant cause in those victims who initially appeared to be free of burns, such as Mr. Tsujimoto, but napalm may well have contributed significantly in many other victims. The use of other poisons is possible but cannot be demonstrated based on the limited evidence available.
| 10.2 |
Acute retinal burns: the dog that didn’t bark |
When exposed to a nuclear detonation, the eyes may be harmed both by the flash of light and by ionizing radiation. The latter most commonly causes cataract, that is, increased opacity of the lens, which typically becomes manifest with a delay of several months or years. An increased incidence of cataract has indeed been repeatedly described in survivors from Hiroshima and Nagasaki; this will be considered in Section 12.3.2. Here, we will focus on the acute lesions that were observed very shortly after the bombing, as well as those that were not observed but should have been.
We have seen earlier that most of the skin burns observed in Hiroshima and Nagasaki were ascribed to the flash of light from the detonation. This raises the question how the same flash would have affected the eyes. The intuitive expectation is that it should have significantly harmed them. Dr. Oughterson thought so, too, according to the ophthalmologist John Flick [193]:
“They say this explosion gives off the light of ten-thousand suns!” he [Oughterson] said to me. “If this be true there should be something for you to do.”
While the ‘ten-thousand suns’ estimate is as vague as it is dramatic—does it refer to overall intensity at some specific distance, or to the maximal brightness of the fireball?—ocular lesions caused by nuclear detonations have indeed been described in both humans and animals.
| 10.2.1 |
Retinal burns observed in humans after later bomb tests |
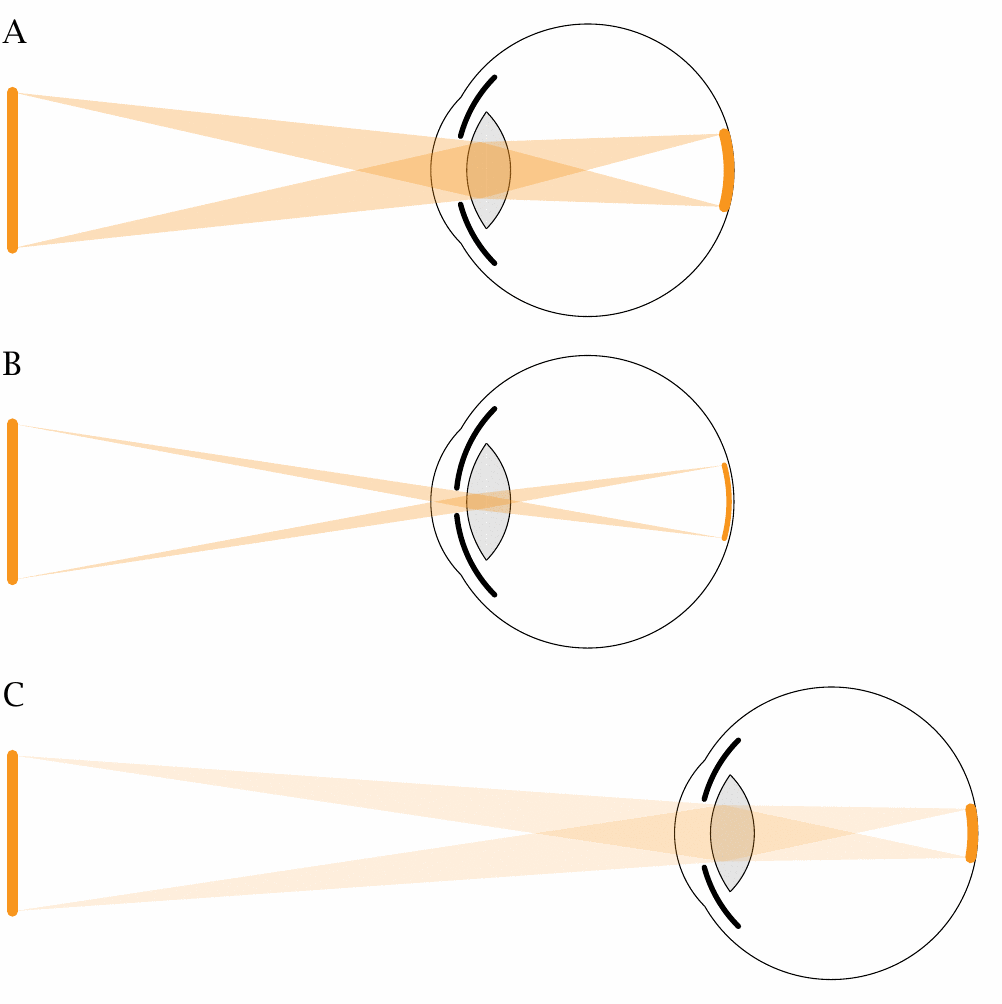
Probably all of us have been warned against looking at a solar eclipse with unprotected eyes. Doing so may cause circumscribed burns to the retina, which will leave behind a permanent defect in the field of vision (a scotoma). The same would be expected in people who happen to look at a nuclear flash, and indeed Rose et al. [194] have reported on six American soldiers who developed just such burns after looking at the fireballs of later nuclear tests, from distances of up to ten miles. The authors also explain why retinal burns may occur at such large distance from the detonations; the reason is illustrated in Figure 10.2. While the light intensity at the pupil decreases with the square of the distance, this effect is exactly compensated by the diminishing size of the retinal image. The brightness of the latter decreases only in proportion to the haziness of the air, which thus becomes the limiting factor.131
The size of the pupil also limits the light intensity at the retina, of course; that is, after all, its purpose. Since the pupil is wider at night than during the day, it follows that retinal burns will occur at greater distances by night. Rose et al. [194] do not provide any details on the time of day or the magnitude of the detonations that occasioned their clinical cases, which means that we cannot directly apply their findings to the conditions at Hiroshima and Nagasaki.
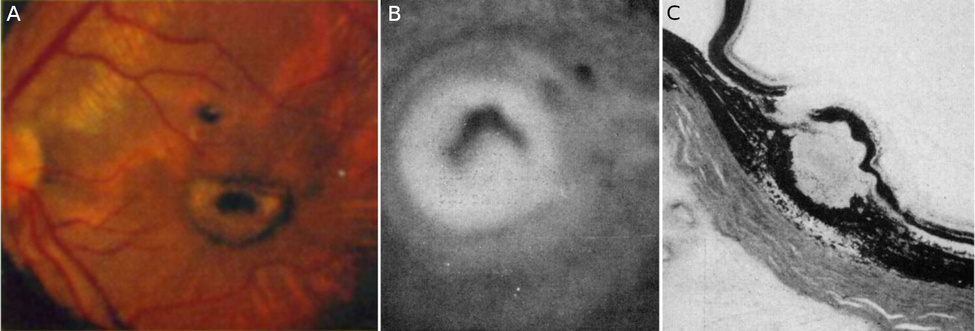
The quantitative aspects of retinal burns are somewhat more explicitly addressed by Byrnes et al. [195]. These authors present studies on 700 rabbits, which were exposed to the flashes of nuclear detonations at night, at distances of up to 42 miles. At all distances, the retinas suffered discrete burns, which with increasing distance decreased in size and in the degree of tissue destruction. Within eight miles of the detonations, the authors describe a ‘volcano-like’ appearance of the lesions,132 with prominent edges and a deep central hole, the bottom of which they made out to be the sclera, that is, the eyeball’s sturdy outer layer of connective tissue. The rabbit eye lesions appear similar to those in Rose’s human patients (Figure 10.3).
Byrnes et al. [195] do not state the magnitudes of the detonations that burned those rabbit retinas. They do, however, apply the findings from their rabbit studies to provide explicit estimates for the range at which a ‘typical’ 20 kt fission bomb—as described theoretically in Glasstone [90], and as purportedly used in Hiroshima and Nagasaki—should cause retinal burns in humans, by day or by night, and under various conditions of visibility. They conclude that the range would be up to 40 miles by night, and some 10-20% less by day. However, they do not spell out all of the assumptions that went into these estimates, and it is not clear to me why the difference in range between day and night would be so small. Their assumed decrease of the pupil aperture from 8 mm by night to 4 mm by day will reduce the energy reaching the retina by a factor of 4; according to my own calculations, this should reduce the range by day to approximately half that by night, giving a maximum range a bit below the atmospheric visibility. Of note, the largest distance among Rose’s case reports [194] is 10 miles.
| 10.2.2 |
Retinal doses of thermal radiation at Hiroshima and Nagasaki |
To gain a firmer footing, we can estimate the heat dose to the retina at Hiroshima and Nagasaki from the thermal radiation which purportedly prevailed on the outside (see Figure 9.1A), the geometrical constraints of ocular vision (see Figure 10.2), and the transmittance of the translucent parts of the eyeball. Following Byrnes et al. [195], the latter will be taken to be 0.4. We will assume a pupil diameter of 2 mm, which corresponds to full adaptation to bright sunlight—the bombings occurred on bright, sunny summer mornings—and a distance from the pupil to the retina of 24 mm.
According to Glasstone [90], the fireball has two distinct stages of high luminosity. The ‘early fireball’ exists at 1 ms after the detonation. It lasts only a very short time, during which a comparatively small cumulative amount of radiation is released; however, its small diameter of only 27 m means that this amount will be focused onto a small retinal image, where the intensity may still reach harmful levels. The late fireball is larger (200-300 m across) and also much longer-lived—up to 3 seconds, but most of the energy is released within the first second. It thus reaches a higher energy density across a larger retinal image. We will consider both stages of the fireball in our calculation.
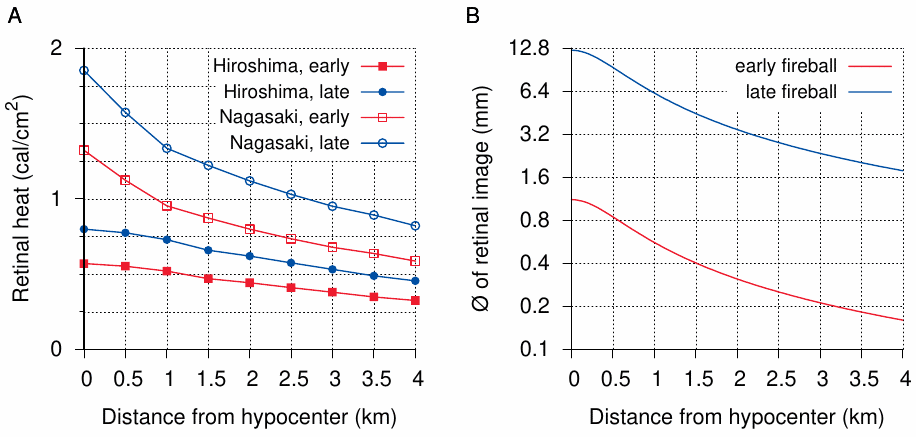
The results are depicted in Figure 10.4. For interpreting them, with need to know the thermal energy which, if transferred to the retina as a very brief flash, will produce a retinal burn. Byrnes et al. [195] estimate this value to be cal/cm2 0.1, and they also state that in a separate series of experiments, which is not described in detail in the cited study (and which I have not found published elsewhere), burns were indeed induced with an only slightly higher energy (cal/cm2 0.14). All data points in Figure 10.4A exceed that threshold.
What are the roles of early and late fireball, respectively, in the generation of retinal burns? On the short time scale of the early fireball (1 ms), no protective lid reflex will be triggered, so that anyone with the flash in their field of vision will receive at least this dose of energy in full. On the other hand, the longer duration of the late fireball means that some of the energy may be shut out by lid reflexes. The question therefore arises to what extent the late fireball contributes to the formation of retinal burns. The sizes of the burns observed by Rose et al. [194], when compared to the predicted ones in Figure 10.4B, suggest that the late fireball does contribute significantly; but since those authors do not tell us how similar those nuclear detonations were in size to the ‘typical’ 20 kt bomb—if they were larger, then maybe so were the early fireballs—we cannot be quite sure. In any event, even in the most stringent scenario—pupils adapted to a bright sky before the flash, and considering the early fireball only—the retinal doses of thermal radiation still exceed the burn threshold. Overall, therefore, both theoretical considerations and previous evidence [194,195] indicate that retinal burns should have been very common in both Hiroshima and Nagasaki.
| 10.2.3 |
Flick’s eye exams in bombing victims |
The ophthalmologist John Flick arrived in Japan in early September and spent several weeks examining a large number of patients in both Hiroshima and Nagasaki. His report [193] is the most comprehensive and detailed of its kind. He writes:
At the end of the second day I had examined approximately 300 patients. I had found the usual traumatic lesions one sees in wartime but none of the corneal or lenticular syndromes I had expected to find. There were few ophthalmias among the sick and those found were of the nonspecific kind due to infection. Knowing the high degree of radioresistance of the tissues of the posterior segment I had paid little attention to ophthalmoscopic studies.133
The posterior segment of the eyeball includes the retina, and its examination uses an ophthalmoscope. Thus, Flick’s remark suggests that he was initially focused on the effects of ionizing radiation more than on those of the flash of light.134 Nevertheless, a short while later, he does make a thorough study of the retinal symptoms in survivors. This is prompted by his observation of retinal bleeding in two patients with hematopoetic syndrome (see Section 8.2.1):
On the third day I was examining two moribund Japanese soldiers with bloody diarrhea, bleeding from the gums, covered from head to foot with petechiae. Their white [blood cell] counts were 2,000 and 900. I examined their eyegrounds. Both had extensive hemorrhagic and exudative lesions of the retina. It seemed entirely consistent with the rest of the picture … these characteristic fundus [retinal] lesions were one of the most reliable criteria of radiation sickness.
In his paper, Flick individually summarizes and also tabulates several dozen of his cases. Of the retinal lesions he describes, he attributes not a single one to ‘flash burn’, nor do any of the lesions shown as illustrations exhibit the striking volcano crater aspect evident in Figure 10.3.
The dearth of clinical cases of retinal flash burn in Hiroshima and Nagasaki is acknowledged by Rose et al. [194], and Byrnes et al. [195]. Both papers do, however, cite one report which purportedly describes one actual case. From Rose et al.:
The literature reveals no report of such a burn except for a single case of bilateral central scotoma incurred in the Hiroshima atomic explosion.
The clinical picture described in the reference given by Rose and by Byrnes, however—Oyama and Sasaki [197]—is not at all characteristic.135 Thus, the medical literature documents not a single case of retinal flash burns in Hiroshima or Nagasaki.
| 10.2.4 |
Pathological findings in the eyes of deceased victims |
Flick shows some histopathological pictures of retinas from deceased patients, which exhibit the sequelae of hemorrhages but again have no similarity with flash burn lesions [193]. Likewise, Liebow, who surveys the autopsy materials he had commandeered from Japanese pathologists while serving on the Joint Commission, mentions hemorrhage as the only type of retinal lesion [42].
Schlaegel has reported a study on autopsy materials from a series of patients at Nagasaki who had died from ‘radiation sickness’ approximately four weeks after the bombings [198]. He finds a variety of lesions, mostly to the anterior eye (see Section 10.3); however, he does not describe or discuss any cases of retinal flash burn. The same is true of another, shorter report by Wilder [199]. Overall, I have found not a single study that provided any evidence of retinal burns in autopsy materials from Hiroshima or Nagasaki.
| 10.2.5 |
Anecdotal reports of retinal flash burns |
In contrast to the medical literature, both Akizuki and Hachiya suggest that some sort of retinal burns indeed occurred. In early September, Akizuki is visited in his hospital by an American military physician, who proceeds to examine the eyes of his patients [167, p. 131]:
He seemed to be an eye specialist, for he began eventually to examine the patients eyes with an ophthalmoscope … The American remarked: “Most of them have had the optic nerves of their retinas damaged by the A-bomb’s flash, and their eyesight has been impaired. They may even lose it altogether.”
Similarly, in his diary entry from August 23rd, Hachiya recounts a conversation with his hospital’s ophthalmologist, Dr. Koyama:
I asked Dr. Koyama what his findings had been in patients with eye injuries. “Those who were watching the plane had their eye grounds burned,” he replied. “The flash of light apparently went through the pupils and left them with a blind area in the central portion of their visual fields. Most of the eye-ground burns are third degree, so cure is impossible.”
On the next day, Hachiya muses about his own condition:
I recalled Dr. Koyama’s account of patients who had been blinded by looking directly at the pika. Their blindness was understandable because their eye nerves had been scorched. My exposure was indirect. I had seen only the flash, but the heat rays had not reached me so the “mirrors” in my eyes were not injured.
Hachiya’s distinction between exposure to the flash and the thermal rays is fictitious, however—‘thermal rays’ may comprise both visible light (‘the flash’) and infrared light, but with a nuclear fireball visible light should account for the greater share. Moreover, both visible and infrared light travel in a straight line; one cannot suffer one but be spared the other.
It is noteworthy that Oyama and Sasaki published their short abstract [197] while employed in the same hospital as Hachiya and Koyama. Presumably, the authors would have had access to the patients examined by Koyama, or at least to their files. In this hospital, a significant number of autopsies were carried out in the weeks after the bombing by Hiroshima medical school pathologist Dr. Tamagawa. His autopsy samples were later appropriated by Liebow, who makes no mention of retinal burns (see Section 10.2.4).
That neither clinical files nor autopsies from Koyama’s own hospital furnished more than Oyama and Sasaki’s single case, which morphed into a ‘retinal flash burn’ only in the skilled hands of later American authors, strongly suggests that Koyama’s diagnosis was premature.136 The cases he observed may have been similar to those which Flick attributed to thrombocytopenia rather than to flash burns, and which would indeed have healed in those patients who survived their ARS in the end. In my view, therefore, the anecdotal reports are lacking in substance and cannot stand up to the uniformly negative evidence from the proper medical literature; they are discussed here only for completeness’ sake.
| 10.3 |
Other acute eye lesions |
Many witnesses describe a ‘blinding flash’, but do not report having been unable to see afterwards. A very bright flash that stays below the burn threshold can indeed transiently suppress our vision; many will have experienced this when exposed to a photographer’s flash.137 In bright daylight, this effect will last a few minutes at most; however, some victims appear to have been blinded for longer periods of time. On August 7th, Hachiya notes in his diary:
I heard footsteps, and a man appeared at the door, outlined in the flickering darkness. His elbows were out and his hands down, like the burned people I had seen on my way to the hospital. As he came nearer, I could see his face—or what had been his face because this face had been melted away by the fire. The man was blind and had lost his way.
Like the case described by Oyama and Sasaki (see Section 10.2.3), this one may have been caused by napalm, but the loss of vision is more acute. Hachiya does not report on the subsequent clinical course in this case. Likewise, he reports once only on another one:
“Has he been fed?” I asked Miss Kado. “Don’t worry, Doctor,” replied Miss Kado. “There are plenty of potato leaves in the garden, so I don’t think he’ll be hungry.”
The patient we were talking about was a horse who had been burned and blinded by the fire. Whoever saw him first did not have the heart to turn him away, so he was put in the garden under our window.
Flick [193] describes a single case of transient blindness which lasted for several days, and which was followed by symptoms suggestive of moderately severe ‘radiation sickness’:
Furuta, a young Nagasaki woman, aged 18 years, was in Ohashi in a wooden house. She states that at the time of the explosion she was blinded and could not see for three days. From August 15th to 18th she had fever up to 40°C. At this time the cuts she had began to be infected. Fever recurred, September 4th to 14th, up to 40∘C, and there was soreness of the gums and tonsillitis.
The combination of symptoms in this case strongly suggests a causation by sulfur mustard (see Section 7.3.3 and 7.3.6). More severe exposure of the eyes to mustard gas can result in the loss of the epithelial cell layers which cover the cornea [109, p. 97]. A similar lesion was described by Schlaegel [198] in one deceased Nagasaki victim (see Figure 10.5). Schlaegel himself ascribes it to ultraviolet rays; however, if UV rays from the flash had indeed been to blame, then the concomitant and much more intense visible light should have caused severe retinal burns as well. Schlaegel also summarizes some clinical observations, related to him by Japanese colleagues, which are entirely consistent with the typical clinical course of mustard gas lesions:
Conjunctivitis and superficial keratitis [inflammation of the cornea] were found in many of the patients, but the effects disappeared in about a month.
On August 24th Hachiya describes another case of blindness in a patient who has been suffering of ‘radiation sickness’:
Mr. Sakai died, complaining of shortness of breath and blindness.
The most likely explanation in this case seems retinal bleeding, as described and explained by Flick (see Section 10.2.3). Overall, therefore, clinical and pathological findings on acute eye lesions don’t provide any specific evidence of eye damage by ionizing radiation or by intense light, while some findings are suggestive of causation by mustard gas or napalm, respectively.
| 10.4 |
Lungs |
| 10.4.1 |
Emphysema and atelectasis in early fatalities |
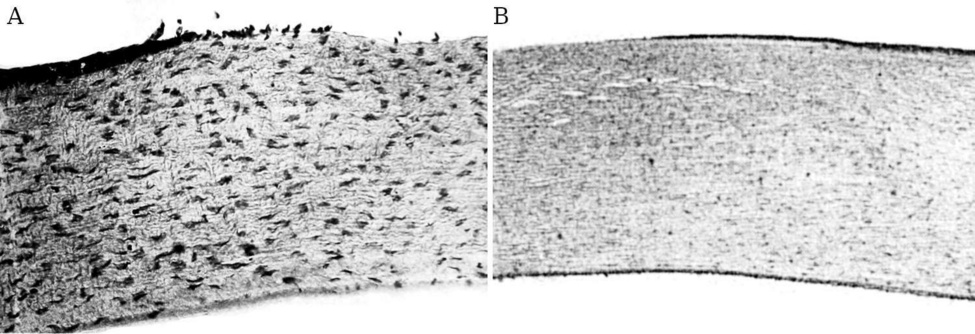
As noted before in Section 10.1.4, the lungs have low radiosensitivity, and they should not have been significantly affected by radiation in any victims that survived the bombing for more than a day. Nevertheless, in the relatively limited number of autopsies that were performed on victims who died within the first one or two weeks, emphysema (distension of lung tissue) was commonly found: Table 8.25 in Ishikawa et al. [8] notes emphysema in 5 patients out of 12 who died between August 9th and 15th, and whose bodies were dissected by the Japanese pathologist Yamashina.
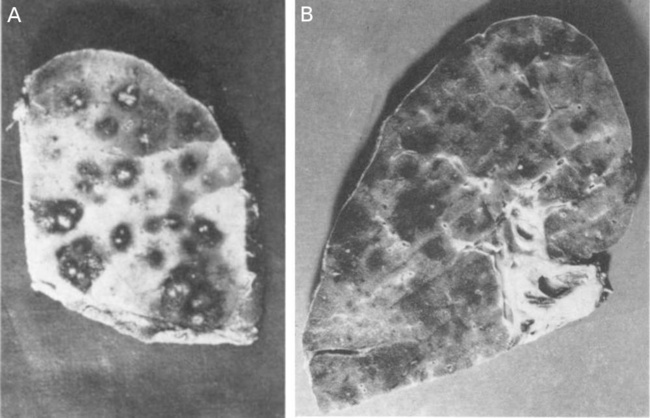
In their loot of Japanese autopsy materials, Liebow et al. [42] also observe emphysema, as well as atelectasis, which is the opposite of emphysema—namely, lung tissue that is devoid of air because it has been cut off from ventilation. They find both in the majority of the limited number of early fatalities they survey. On page 856, they note:
The foci of pulmonary emphysema and atelectasis without hemorrhage observed in some of the early casualties (Fig. 20) are difficult to interpret. These were found frequently at death in patients who had not been exposed to blast.
Liebow’s Figure 20 (referred to in the quote) is shown here as Figure 10.6. The deceased patient is a thirteen years old boy, who is said to have died on the third day; thus, the lesions are truly acute and indicate some sort of obstruction of bronchioles (small bronchi).138
The difficulty which Liebow and colleagues perceived with interpreting their findings is readily dispelled if we consider causes other than atomic bombs. The book “The residual effects of warfare gases” discusses the effects of mustard gas on the lungs and observes [139, p. 92]:
Emphysema was frequently found in combination with bronchitis. It usually appeared immediately after gassing and was compensatory in character, due to the extensive atelectasis found following gassing with mustard.
The atelectasis, in turn, is understood to arise from bronchial obstruction. Thus, what we have here is a milder expression of the pathological changes in the lung which we invoked in Section 10.1.4 to account for the clinical picture in immediate fatalities on the day of the bombing.
| 10.4.2 |
Focal and confluent hemorrhage, inflammation, and necrosis of the lungs in later fatalities |
The largest group of patients whose autopsy materials were surveyed by Liebow et al. were those who had succumbed within weeks 3 to 6 after the bombing. In slightly more than half of these cases, the authors found a varied picture with edema, hemorrhage, necrosis, and infection. These processes were focused on the bronchioles (small bronchi) but tended to expand and become confluent (see Figure 10.7).
With respect to this group of patients, Liebow et al. don’t express any puzzlement as to the causation; presumably, they ascribe their findings to the bone marrow suppression, which would pave the way for infections and also for the hemorrhage. This is indeed most likely an important contributing factor, and it would be equally well explained by radiation and mustard gas. We may note that the lesions remain centered on the bronchi, which suggests primary damage to them; this would be expected with mustard gas, yet not impossible in its absence. The same combination of findings was reported in a series of autopsies of German mustard gas victims (from the final months of World War I) by Heitzmann [28]. In summing up his findings, Heitzmann describes the appearance of the lungs as bunt, that is, checkered, which seems an apt description of the lungs shown in Figure 10.7. On the other hand, high-dose irradiation alone did not cause any of these changes in animal lungs [26, p. 704 ff]. Overall, while Liebow’s findings suggest causation by mustard gas rather than by radiation, the time elapsed between trauma and death means that this evidence is more ambiguous than the atelectasis and emphysema at the very early stage.
| 10.5 |
Neck organs |
In most of the cases surveyed by Liebow et al. [42], death occurred in or after the third week. Therefore, as with the lung pathology in the preceding section, it can be difficult to distinguish primary damage from secondary effects of bone marrow suppression, which facilitates severe infection in these locations and would by the third week have reached its peak. In some of their cases, however, they do describe and depict injury that is predominantly necrotic—that is, due to direct damage by either radiation or mustard—rather than infectious. This is particularly clear in their single reported case of early death, a young man of 19 years who died on the tenth day and who is listed in their records as ‘K-98’. Concerning this case, the authors note:
In the records of the necropsies of 2 individuals, K-98 (group I) and K-109 (group II), who were recently dead, the skin was said to have “peeled” easily revealing a pink raw surface beneath. The tongue, pharynx, and esophagus of one of these patients, K-98, showed remarkable changes in the epithelium with sloughing over large areas.
Later on, they remark that “the changes in the tissues of K-98 undoubtedly represent radiation effects.” Of course, these findings represent anything but radiation effects, since all of the epithelial tissues in question are quite radioresistant and thus should not have been destroyed by radiation more severely than any others; and it is hard to believe that Liebow and particularly his co-author Warren, who had been studying these matters for many years, would not have known this. Instead, both the peeling skin and the necrotic mucous membranes of the pharynx and esophagus are perfectly typical of mustard gas exposure. The authors also note that bone marrow damage has already set in, which rounds out the picture.
| 10.6 |
Gastrointestinal tract |
The experimental studies reported by Bloom [26] indicated that among the intestines the duodenum (i.e., the uppermost part of the small intestine) is the most susceptible to both radiation and sulfur mustard. However, it is likely that in their studies on mustard gas they applied the poison by intraperitoneal or intravenous injection, so that the gastrointestinal tract would have been affected by way of the bloodstream, causing an equable exposure of all segments.
We had already seen in Section 8.10 that early and violent diarrhea was common among the bombing victims. The most likely explanation is that they had ingested food or water contaminated with mustard gas. In such a case, we might expect that the toxic effect will be most pronounced in those bowel segments within which the ingested food and fluids dwell and stagnate the longest. Within the small intestine, this is the lowermost part, whose emptying into the large intestine is controlled and delayed by the ileocecal valve [200]. It is interesting, therefore, that Liebow et al. [42] note:
In the small intestine also there were foci of necrosis, usually discrete. They were most numerous in the region of the ileocecal valve where there was almost always involvement.
The authors show several pictures of necrotic ileocecal valves and adjoining segments of small and large intestine, in which exposure to ingested mustard would have been prolonged by generally slow transport of bowel content. Likewise, the stomach is strongly affected, although from the descriptions of these lesions it is again difficult to distinguish direct effects from those facilitated by bone marrow failure.
An interesting episode of gastrointestinal affliction is related by Hachiya [62]. Having recovered from his initial illness and injury after several weeks, he leaves his hospital to visit friends in downtown Hiroshima. On his return, he suffers violent diarrhea, initially watery but later bloody. On the next day (September 24th), he muses:
I wondered if I had inhaled the ‘bad gas’ people spoke about, during my wanderings in the ruins yesterday? 139 The next time the amount was less, but mucus was present and tenesmus greater.
Considering that his symptoms are gastrointestinal rather than respiratory, it seems more likely that he has ingested rather than inhaled the poison. On September 29th, he notes:
I passed a plug of mucus about ten centimeters long and cylindrical in shape, with surface markings like a casting of intestinal mucosa. I was not a little startled to see this, and on examining it closely was convinced I had had a mucous enteritis rather than radiation sickness.
Even though Hachiya refers to it as mucus, the plug must have consisted of some firmer material, since mucus would be too soft to retain a specific three-dimensional shape during passage through the anal sphincter. Indeed, his description evokes the fibrin casts that form within bronchi whose blood vessels leak blood plasma into the luminal space after having been scoured by sulfur mustard (see Section 7.3.2).
| 10.7 |
Other organs |
Most of the other organs affected in the bombing victims were exposed via the bloodstream rather than directly. In many of these, such as the bone marrow, spleen, and gonads, the pathological findings will indeed be similar between mustard gas and radiation, with severe depletion of the respective organ-specific cell types. Predictably, these are the organs that Liebow et al. [42] like to dwell on. In the early reports by the Japanese pathologist Yamashina (listed by Ishikawa et al. [8] in their in Table 8.25)—which were completed before Japan’s capitulation, and thus before Liebow and his colleagues could lay their hands on the autopsy materials—the liver is more prominently afflicted than one would expect with radiation, based on the mostly negative findings from experiments that exposed animals to high radiation doses [26, p. 541 ff]. Yamashina’s observations—congestion, cloudiness, fatty liver—are compatible with findings reported in mustard gas poisoning [17] but are not specific for this condition. Overall, a more detailed examination of further organs appears unlikely to add significant weight to the evidence in our case and will therefore be omitted.