| 9 |
Skin burns in survivors |
The literature ascribes most of the burns observed in survivors of the ‘atomic’ bombings to the flash of the detonations. It will be shown here that this interpretation meets with numerous difficulties:
- In Hiroshima, the incidence of severe burns was greatest at a distance of between 2 and 2.5 km from the hypocenter. At this range, the intensity of the flash should have been only 1/8 of that at a distance of 1 km.
- Many ‘flash burns’ occurred in skin areas covered by clothes, and in some cases even underneath clothes that remained intact after the ‘flash’.
- The outlines of hypertrophic scars (keloids) left behind by the burns are often discontinuous and completely irregular—partial shielding by clothes cannot explain such patterns.
- Proper flash burns should be manifest immediately. While this is indeed true for some of the observed burns—presumably those caused by napalm—others became manifest only after a significant delay, which is typical of the chemical burns caused by mustard gas.
Overall, therefore, the evidence clearly rejects the traditionally accepted interpretation of survivors’ burns as ‘flash burns’. In contrast, the observations are well explained by the combined effects of napalm and mustard gas.
Disfiguring scars of the skin have a prominent place in Hiroshima and Nagasaki lore. These lesions are mostly ascribed to the ‘flash burns’ caused by light from the ‘ball of fire,’ which is said to have formed during the first second of the nuclear detonation [90]. One might wonder why, among the various physical effects accompanying a nuclear detonation, only the flash of light is considered in this context. Can we rule out ionizing radiation as a possible cause of skin burns?
When animals are experimentally irradiated with γ-, X-, or neutron rays at doses that are lethal due to their effect on the bone marrow or other sensitive organs, the skin nevertheless shows little evidence of injury [26, p. 44 ff.]. Thus, if someone survives a nuclear detonation by 20 days or beyond, as is the case with the group of victims surveyed by the Joint Commission [33], we can infer that any major skin burns could not have been caused by γ- or neutron rays from the bomb. Preferential damage to the skin can indeed be brought about by β-rays (see [26] and Section 2.7.1). Radionuclides in the fallout must have given off some β-radiation, but only at levels too low to cause acute injury.110 Thus, the only mechanism that remains for the causation of skin burns by nuclear bombs is indeed thermal radiation.
It is worth noting that a nuclear detonation releasing a flash of light as intense as purportedly occurred in the bombings should indeed have caused flash burns. This is confirmed by experimental studies, some of which are discussed in Section 9.6. However, as we will see in this chapter, many features of the observed burns show that they cannot have been caused in this manner; the evidence points instead to napalm and to mustard gas as the true causes of many of these burns.
| 9.1 |
Classification of skin burns |
Before we dig into the evidence, a few words about terminology are in order. Skin burns can be classified according to the cause and, independently, according to severity.
| 9.1.1 |
Causes of burns |
These include contact (hot objects or liquids, napalm), chemicals (sulfuric acid, mustard gas), and thermal radiation. Although all of the major causes that we will consider here—flash burns, napalm, and mustard gas—fit into this classification, they all differ from more commonplace causes encountered in everyday life.
Mustard gas burns develop more slowly than those with some widely used caustic chemicals, such as strong acids (sulfuric or hydrochloric acid) or bases (lye). The delayed onset of its effect makes mustard gas particularly treacherous. This is illustrated by the casualties of the Bari incident (Section 1.4.5): the victims did not perceive any pain shortly after exposure, and many neglected to change their contaminated clothes before the night, only to awake to severe skin burns on the morning after [22].
Napalm burns may be classified as contact burns. However, in this case the combustible material is designed to stick together in sizable chunks that adhere to target surfaces [141], which means that the amount of heat transferred to those surfaces will be unusually high. Thus, compared to conventional contact burns, napalm burns tend to be particularly severe [142,170].
Nuclear flash burns are a special case of burns caused by thermal radiation. Here, the energy is delivered in a particularly brief and intense pulse, which means that the heat absorbed by the skin has no time to dissipate toward the tissues beneath, but instead causes very high temperatures within a thin superficial layer. Investigators have found ways to emulate such high intensity flashes; the results of some such studies are detailed in Section 9.6.
| 9.1.2 |
Severity of burns |
Burn severity is expressed in degrees:
- first degree burns show irritation and erythema (reddening), but no damage to the anatomical skin structure;
- in a second degree burn, a superficial layer of the skin detaches to form a blister. Usually, the skin underneath can regrow from deep-set patches within hair follicles or sweat glands and heal quickly, with minor scarring or without it;
- a third degree burn destroys the entire depth of the skin. The wound is closed by new skin growing inwards from the periphery, and a scar will form;
- a fourth degree burn includes significant injury to tissues beneath the skin.
All manifest burns should be painful to some degree. Volunteers who received experimental first or second degree flash burns uniformly reported instantaneous pain (see Section 9.6). Third and fourth degree burns will destroy the nerve endings of the skin together with the skin itself, which may alter pain quality and intensity; however, as long as the victims remain conscious, they should still perceive some sort of pain, originating from pain receptors in the most superficial layer of tissue that remains viable. With chemical burns, however, pain will often not be perceived in the instant of contact with the chemical, but only after the chemical has penetrated the skin and a damaging chemical reaction has had time to occur. As noted above, with mustard gas in particular the manifestation of visible lesions and the perception of pain tend to be delayed.
| 9.2 |
Statistical observations on burns in Hiroshima and Nagasaki |
| 9.2.1 |
Flash burns vs. flame burns |
When the survivors studied in each city by the Joint Commission (see Section 8.4) were grouped by distance from the hypocenter, the highest incidence of burns of any kind in any of the groups was 47.3% (see Tables 8H and 8N in [33]). Up to 1.4% of all victims were diagnosed with only flame burns, and up to 32.6% with only flash burns. Up to 7.3% were listed with both flame and flash burns, while the cause of the burns was stated as unknown in 9% of all cases. Thus, the majority of burns were considered flash burns, but the presence of some putative flame burns must be kept in mind.
| 9.2.2 |
Observed incidence of burns by distance from the hypocenter |
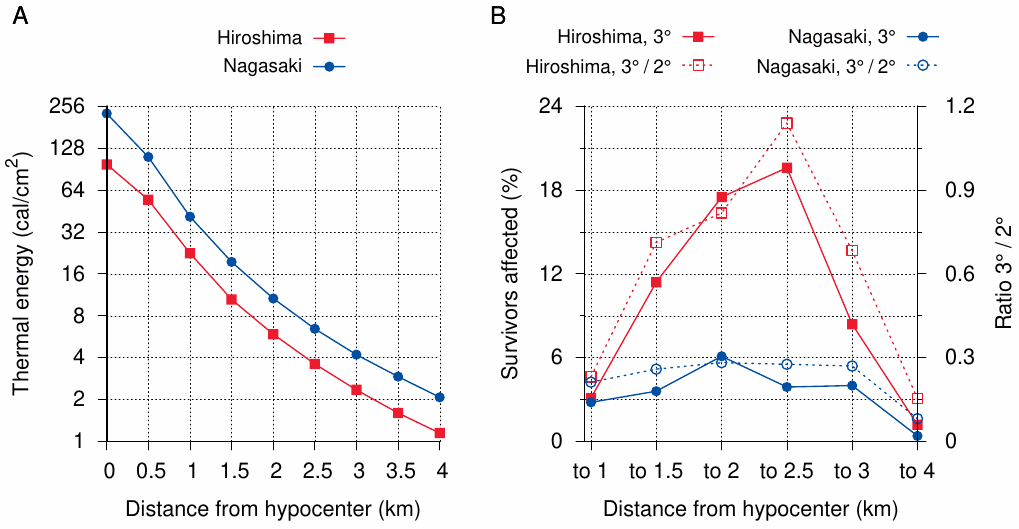
Figure 9.1 A shows the intensity of the thermal radiation as a function of distance from the hypocenters.111 Within 1 km of the hypocenter, these intensities would have exceeded anything that has been tried in experiments on human volunteers or animals (see Section 9.6); however, we can extrapolate that such doses should cause burns of at least the third degree. Overall, considering the postulated intensities and the experimental findings, we should expect the following features in the distribution of flash burns about the hypocenter:
- the number and severity of flash burns should have been greatest near the hypocenter. With increasing distance from it, both incidence and severity should have decreased;
- within 1 km of the hypocenter, most flash burns should have been of third or fourth degree. Lower degrees should only have occurred with attenuation by at least two layers of clothing or some equivalent partial protection;
- burns should have been more severe in Nagasaki than in Hiroshima, or at least not less so.
Figure 9.1 B shows that none of these expectations corresponds to observation. The incidence of third degree burns grows from the hypocenter towards a maximum at 2 or 2.5 km, respectively. In Hiroshima at least, this increase is so pronounced that it cannot plausibly be explained by the statistical noise from flame burns.112 To judge burn severity, we can look at the ratio of third degree burns to second degree burns. In Hiroshima, this ratio also increases substantially between 1 and 2.5 km. In Nagasaki, neither trend is very pronounced, but both the incidence of third degree burns and the burn severity are strikingly lower than in Hiroshima, even though the bomb yield, and therefore the thermal radiation, are said to have been greater in Nagasaki.
| 9.2.3 |
Flash burns in skin areas covered by clothes |
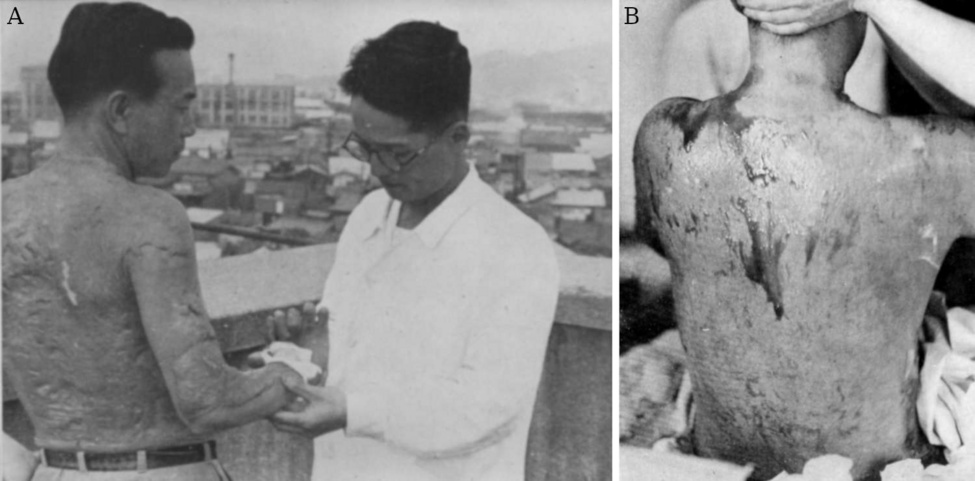
Clothes should afford partial protection from flash burns (see Section 9.6). Since dark clothes will absorb heat more readily than white or light ones, we might expect flash burns in covered areas to be more common with dark clothes. The numbers stated in Table 13 in [33] support such a relationship: those wearing colored clothes more often had burns in covered areas in addition to uncovered ones.113 With neither white nor colored clothes, though, should we expect any burns to occur in the covered areas only, without any burns in the exposed skin. However, the scars left by just such a burn are seen in Figure 9.2 A. The scars cover almost the entire upper body and the arms of the victim, but none are visible above the collar line. A strikingly similar distribution is observed in panel B, which shows a victim of mustard gas exposure; we note only some dark pigmentation, but no deep lesions on the back of the neck.114 For further examples of the same effect in alleged nuclear flash burns, see [77,169,172]. Moreover, Oughterson et al. [33] state in their Table 13 that 5.4% of all burn victims in Hiroshima, and 9% of those in Nagasaki, had burns in the clothed area only.
Whatever the color or thickness of the clothes, they would have to be burned away by the radiant heat first in order to reach the skin underneath. Nevertheless, some burns apparently occurred underneath the intact clothing. Eyewitness Mr. Hashimoto relates giving first aid to a girl with burns on her backside, as quoted by Hachiya [62]:
I … began painting [with mercurochrome] the wounds of a girl dressed in monpe [pants] … Her wounds were mostly on her buttocks and these I found hard to bandage, for when she stood up the bandage slipped off. … Finally, I gave up and in desperation pulled down her monpe, and after repainting her wounds, pulled up her monpe and put the bandages on right over them.
From this account, it is quite clear that this girl still had her pants, yet had suffered burns underneath them, in a location that is commonly affected by sulfur mustard, as moist skin areas generally are (see [109] and Figure 7.6).
Finally, while I have not seen any experimental studies on the subject, I surmise that the layer of sturdy hair that covers the skin of a horse should provide substantial protection from flash burns. Nevertheless, there are multiple reports of horses having suffered burns as well, for example this one by eyewitness Akihiro Takahashi [156, p. 193]:
… a horse, only raw flesh, lying dead with its head in a cistern.
While we cannot be sure about the cause of such burns in every single instance, a plausible one is mustard gas, which should penetrate hair and fur just as readily as it penetrates clothing. Mustard gas lesions in horses were indeed noted in World War I (see Figure 7.6). Overall, therefore, the manifestations of burns in covered skin observed in Hiroshima and Nagasaki do not fit the pattern expected of true flash burns.
| 9.2.4 |
Irregular shapes of flash burns |
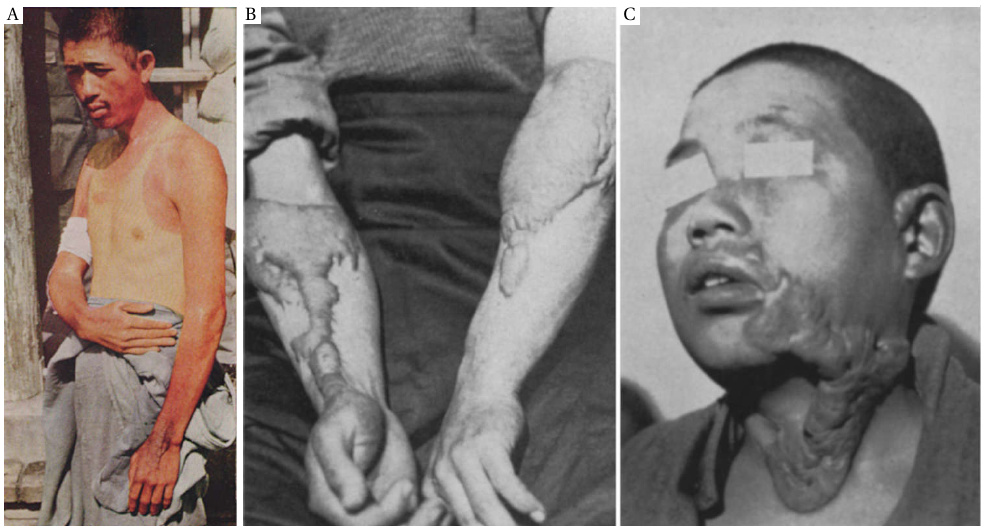
Much like a sunburn, a flash burn should affect the exposed areas of skin quite evenly. Figure 9.3 A shows the expected distribution; however, part of the skin shows fresh erythema, even though this picture was taken only on October 11th, that is, more than two months after the bombing. While experimental flash burns of low or moderate severity indeed initially manifest as erythema, they progress within days either to heal without defect, or to first shed the damaged skin and then heal, possibly with some degree of scarring (see Section 9.6). Thus, the erythema visible on October 11th could not have been caused by the bombing on August 6th. We can speculate, but cannot prove, that this fresh sunburn was staged and photographed as a welcome present for the Joint Commission that arrived in Hiroshima on the following day.
Panels B and C of Figure 9.3 show keloid or hypertrophic scar tissue formed in lesions ascribed to flash burns.115 The lesions have highly irregular shapes that cannot plausibly be explained with any sort of partial cover by clothing or shielding. Nevertheless, such irregular shapes are typical of ‘flash burn’ illustrations in both general and medical references; the more regular pattern shown in panel A is the exception.116
The irregular shape was noted by early observers. Shigetoshi Wakaki, a Japanese military officer who was involved in weapons research and development, and who entered Hiroshima shortly after the bombing, notes [173, p. 88]:
The greater the distance from the centre, the greater the proportion of those who had freckle burns.117 This made it difficult to explain the burns simply by radiant heat … at least some part of the cause was something other than radiant heat.
Additional evidence to prove that the lesions could not possibly have been caused in the claimed manner will be introduced in Section 10.2. For now, we will dismiss the idea of nuclear flash burns and turn to the more interesting question of what the real causes of the observed burns may have been.
| 9.3 |
Fast and slow burns |
If one surveys multiple eyewitness reports, a dichotomy emerges between burns that became manifest immediately after the bombing and those that developed more slowly. We will here quote one illustrative example for each. Sumiteru Taniguchi of Nagasaki [156, p. 113] suffered burns immediately:
The wind from the blast, coming from behind, hurled me and my bicycle to the ground … I think two or three minutes passed before the earth stopped trembling and I heaved myself up. … The skin of my left arm had peeled from the upper arm to the tips of my fingers and was hanging in strips. When I felt my back and buttocks, I found that the skin there had been burned to a pulp and that only the front part of the clothes I had been wearing remained.
The burns to Taniguchi’s backside were indeed extensive (see Figure 9.4 B), and he had to lie with his face down for more than a year until the wounds finally began to heal, ultimately with severe scarring and keloid formation.

An instance of delayed skin injury in a bombing victim is described by the physician Michihiko Hachiya [62]. In his diary, he notes between August 6th and August 8th:
- (6th) I opened my eyes; Dr. Sasada was feeling my pulse. What had happened? … I must have fainted.
- (7th) Dr. Sasada, who had looked after me yesterday, lay on my left. I had thought he escaped injury, but now I could see that he was badly burned. His arms and hands were bandaged and his childish face obscured by swelling …
- (8th) Dr. Sasada’s face was more swollen this morning than yesterday, and blood-stained pus oozed from his bandaged arms and hands. I felt a wave of pity when I thought how he had used those hands to help me two days ago.
Further on in his diary, Hachiya reports how Dr. Sasada later develops symptoms of bone marrow suppression, but ultimately recovers. From Hachiya’s description, it is apparent that Sasada’s hands were injured not in the bombing itself; he could not have felt Hachiya’s (presumably faint and rapid) pulse with wounded, bandaged hands. His burns sprung up only after he had tended to many victims who, like Hachiya himself, had been more severely injured outright.118
Mr. Taniguchi’s immediately manifest burns and tattered clothes strongly suggest that he was hit directly with some sort of incendiary, most likely napalm. In contrast, the most straightforward explanation for Dr. Sasada’s delayed burns is that, by touching the skin and clothes of his patients who had been contaminated with sulfur mustard, he was himself exposed to toxic quantities of it. His swollen face and subsequent symptoms of bone marrow suppression are likewise suggestive of mustard gas exposure.
The limited available data do not permit us to estimate the relative abundance of each type of burn; we will therefore merely discuss qualitatively the evidence which leads us to attribute them to napalm and to mustard gas, respectively.
| 9.4 |
Evidence of napalm burns |
According to his description of his own travails on August 6th, Hachiya himself, like Mr. Taniguchi, was most likely burned by napalm, possibly with some additional mustard lesions as well. As he struggles towards the hospital, bereft of his clothes, he observes:
Others moved as though in pain, like scarecrows, their arms held out from their bodies with forearms and hands dangling. These people puzzled me until I suddenly realized that they had been burned and were holding their arms out to prevent the painful friction of raw surfaces rubbing together. A naked woman carrying a naked baby came into view. I averted my gaze. Perhaps they had been in the bath. But then I saw a naked man, and it occurred to me that, like myself, some strange thing had deprived them of their clothes.
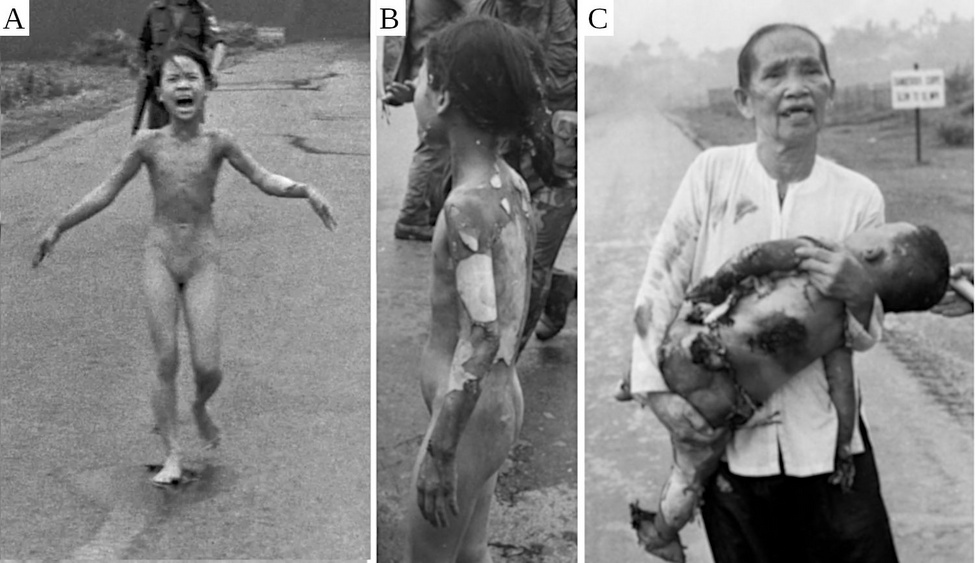
Have we seen something like this anywhere else? Considering the widespread use of napalm—large amounts were dropped on Japan, and even larger ones on Korea and Vietnam—generally accessible information on napalm is extremely scarce (see Section 7.4). However, there is one very widely known picture of a napalm victim: Kim Phuc, a Vietnamese girl who in 1972 suffered burns when her village in South Vietnam was attacked by the country’s own air force (the village had been infiltrated by the Vietcong). This picture (Figure 9.5 A) shows her running in the nude, in the ‘scarecrow’ posture also described by Hachiya. The real extent of her burns is only visible from another angle (Figure 9.5 B), which also reveals the immediate peeling of the skin. Peeling and flapping skin are likewise apparent in Kim’s even more severely burned cousin Danh (Figure 9.5 C). While the little boy died within an hour of the attack, Kim survived. Even with expert surgical treatment, however, her burn wounds turned into extensive scars that resemble the keloids shown in Figure 9.3.
The pronounced tendency of ‘nuclear flash burns’ to heal with keloid formation has often been noted; Harada [174] cites figures of > 70% for burns and > 20% for injuries from a reference in Japanese. The same is true of napalm burns. According to the Russian physician Plaksin [142], keloid formation was observed in 52.7% of all patients in a series of 1026 Korean napalm burn patients. The author ascribes this to the high amount of heat transferred from the burning napalm to the adjacent tissues.

While pictures of victims with ‘nuclear flash burns’ abound, those of napalm burns from conventionally firebombed Japanese cities such as Tokyo are surprisingly hard to find, even though survivors with napalm burns should have been common enough. I have only found one such picture, which is shown here as Figure 9.6. According to the source [169],119 the victim was burned in an incendiary bombing raid on Tokyo when burning napalm hit a nearby fuel barrel, causing it to explode. The effect of burning gasoline on the skin would have been similar to that of burning napalm itself. The authors state explicitly that his lesions were ‘entirely comparable’ to those in atomic bomb survivors, and also that they saw more than twenty similarly afflicted bombing victims from Tokyo. In all likelihood, at least some of those patients had been struck by napalm directly rather than by burning gasoline.
In summary, the evidence strongly suggests that those of the burns in Hiroshima and Nagasaki that were manifest immediately, accompanied by burning and stripping of clothes, and followed by keloid formation, were caused by napalm. While rare, explicit accounts of exposure to napalm or a similar substance can indeed be found. John Toland [76, p. 803] relates this experience of a boy in Nagasaki:
Hajime Iwanaga, who would be fourteen the next day, was bathing in the Urakami River near the torpedo factory. He … exuberantly ducked his face in the water as the pika120 flashed. Seconds later he emerged into a blinding world. Something warm clung to his left shoulder. It was yellowish. Mystified, he touched it and saw skin come off. He splashed toward the bank as the sky darkened ominously, and was reaching for his clothes when two dark-green spheres, the size of baseballs, streaked at him. One struck his shirt, set it afire, and disintegrated.
Those green spheres carried fire, but did apparently not cause any harm through kinetic impact, which means that they consisted of some soft, incendiary material, much like napalm. The material on the shoulder may have been a chunk of napalm, too, that was extinguished when the boy dived underwater. For comparison, here is Kim Phuc’s recollection:
Her first memory of the engulfing fires was the sight of flames licking her left arm, where there was an ugly, brownish-black gob. She tried to brush it off, only to scream out at the pain of the burn that had now spread to the inside of her other hand.
In both cases, the size and texture of the lumps of incendiary material described are consistent with those of napalm [141].
| 9.5 |
Chemical burns by mustard gas |
In Section 1.4, we noted the similarity of skin lesions described by John Hersey in victims of the Hiroshima bombing to those observed by Alexander [22] in the mustard gas casualties at Bari. Eyewitness testimony from Hiroshima and Nagasaki further suggests that chemical burns to the skin by mustard gas were common. Kiyoko Sato, a girl from Hiroshima, had been evacuated to the countryside and returned to the city about a week after the bombing. Upon arrival, she finds her mother just a few moments after she has died [156, p. 55]:
If I had only walked a little faster, I would have been in time! I was distressed that I had not been able to see her alive and cried loudly. My mother’s face was covered in blisters and had swollen to twice its normal size, and her hair had fallen out. She was unrecognizable as the mother I had known so well.
A boy from Nagasaki, Yoshiro Yamawaki, walked across the city in search of his father on the day after the bombing, together with his twin brother [175]:
There were many dead bodies amongst the debris littering the roads. The faces, arms and legs of the dead had become swollen and discolored, causing them to look like black rubber dolls. As we stepped on the bodies with our shoes, the skin would come peeling off like that of an over-ripe peach, exposing the white fat underneath.
Neither witness mentions any scorching of the dead bodies in question, and both descriptions match the known appearance of mustard gas burns.121 We already noted above instances of burns becoming manifest only on the next day or occurring under clothing that remained intact; neither incendiaries nor flash burn can account for these observations. Having already considered the evidence that points to mustard gas as the cause of ‘radiation disease’, we now see that the expected skin lesions were prevalent also.
| 9.6 |
Appendix: experimental flash burns to the skin |
The light intensities assumed to have been released by the bombings in Hiroshima and Nagasaki are shown in Figure 9.1 A. The surface temperature of the ‘ball of light’ at its most luminous stage should be in the range of 5000-7000 °K [90], which is similar to that of the sun. Therefore, the supposed atomic flash can be likened to a brief, intense pulse of sunlight, with similar proportions of ultraviolet, visible, and infrared light.
A number of experimental studies on animals and on human volunteers have attempted to model the flash burns produced by nuclear bombs. In a study on dogs [176], a thermal dose of cal/cm2 8 was applied to 20% of the body surface. Figure 9.1 A shows that this intensity is well within the range of intensities expected near the hypocenter. Mortality was relatively low (2 dogs out of 30) and due to septicemia. The wounds appeared different from those caused by contact burns:
Following a flash burn of the magnitude given in this study, an eschar is formed on the burned surface. … This initial eschar persists throughout … Healing of the flash wound was usually complete by four weeks with the eschar acting as a protective dressing for epithelization from deep hair follicles and wound edges.
These results suggest that peeling of the skin might not occur in nuclear flash burns. However, blistering lesions were observed in an experimental study on human volunteers [177]. At sufficiently high doses, a superficial skin layer came off one or two days after the irradiation and left behind a red, moist wound, which does resemble the observations of peeling skin in the bombing victims. This study reports several more pertinent observations that we can compare with those made in those victims:
- A dose of cal/cm2 2 produced only a transient erythema, which typically subsided within half an hour. This represents a first degree burn.
- With doses of cal/cm2 3.9 and above, erythema of the lesion itself was immediate, and it persisted until it gave way to blisters, whereas the vicinity of the lesion showed delayed and transient erythema. Thus, any lesions of at least second degree are visible in some form immediately and throughout.
- The maximal dose given—cal/cm2 4.8—produced at least second degree burns in all volunteers, and third degree burns in some.
- While for obvious reasons the experimental flash burns were small (1.25 cm in diameter), it nevertheless was evident that the entire light-exposed area was evenly burned.
- The volunteers reported immediate pain, which was described as sharp or stinging and increased with the intensity of the flash.
Clothes should offer some protection against flash burns, although it is conceivable that at very high intensity the clothing might burn up, and enough heat might be left over to damage the skin underneath. A study by Mixter [178] used an animal model (pigs) to compare the doses required to set burns in nude skin to those required with skin areas covered by one or by two layers of fabric, respectively. With nude skin, the doses determined by Mixter are similar to those that had been determined in humans by Evans et al. [177].
While Mixter’s data on the effect of clothing show some scatter, a reasonable approximation is that each layer of fabric raises the energy threshold for a burn by a factor of 2.5. Thus, burns beneath two layers of fabric—which can be assumed to have been present in most victims at least around the hips—would require about 6 times more energy than on exposed skin.