Michael Palmer, MD and Sucharit Bhakdi, MD
Winston Churchill
1. Background
On August 29, 2023, Ivan Vilibor Sinčić, a Croatian member of the EU Parliament, posed the following simple and poignant question to the EU Commission:
On November 6, he received the following written reply from Ms. Stella Kyriakides, the EU Commissioner for Health and Food Safety:
Scientific studies investigate potential causal links in these temporal associations and most suspected side effects are not eventually confirmed as side effects.
An unprecedent [sic] high number of people has been administered COVID-19 vaccines [1] and the number of reported suspected side effects is consequently much higher than for other medicines.
As of 30 September 2023, EudraVigilance shows 11,977 spontaneous reports of suspected side effects with reported fatal outcome for all authorised COVID-19 vaccines.
Only in very exceptional cases, deaths have been reported to be caused by the vaccine. One example is ‘thrombosis with thrombocytopenia syndrome’ with adenoviral vector COVID-19 vaccines [2] for which warnings and contraindications have been included in the product information to inform healthcare professionals and patients and reduce risk of adverse consequences.
There is no evidence that COVID-19 vaccines are causing excess mortality [3] and no safety signal for increased mortality with any of the authorised COVID-19 vaccines has been identified by EMA to date. In fact, COVID-19 vaccines have saved millions of lives.
[1] Almost 768 million vaccine doses administered in EU and EEA countries.
[2] https://www.nature.com/articles/s41541-022-00569-8
[3] https://www.icmra.info/drupal/strategicinitiatives/vaccines/safety\_statement
In this memo, we will dissect and rebut the position stated by Ms. Kyriakides on behalf of the EU Commission and of the European Medicines Agency (EMA).
2. What significance should we assign to adverse events reported in connection with COVID-19 vaccination?
Ms. Kyriakides observes that the filing of an adverse event report alone does not prove causality in this specific single case. This assertion is hardly controversial. However, should we therefore dismiss the many adverse events, including severe and fatal ones, which have been reported to EudraVigilance and to similar monitoring systems around the world?
2.1. Is the high number of reports simply due to the widespread use of the COVID-19 vaccines?
In her reply, Ms. Kyriakides suggests that the high number of adverse events reported for the COVID-19 vaccines is due simply to the large number of injected doses. This raises the question of relative risk: is a single dose of a COVID-19 vaccine equally likely, less likely, or more likely to result in an adverse event report than a dose of a conventional vaccine?
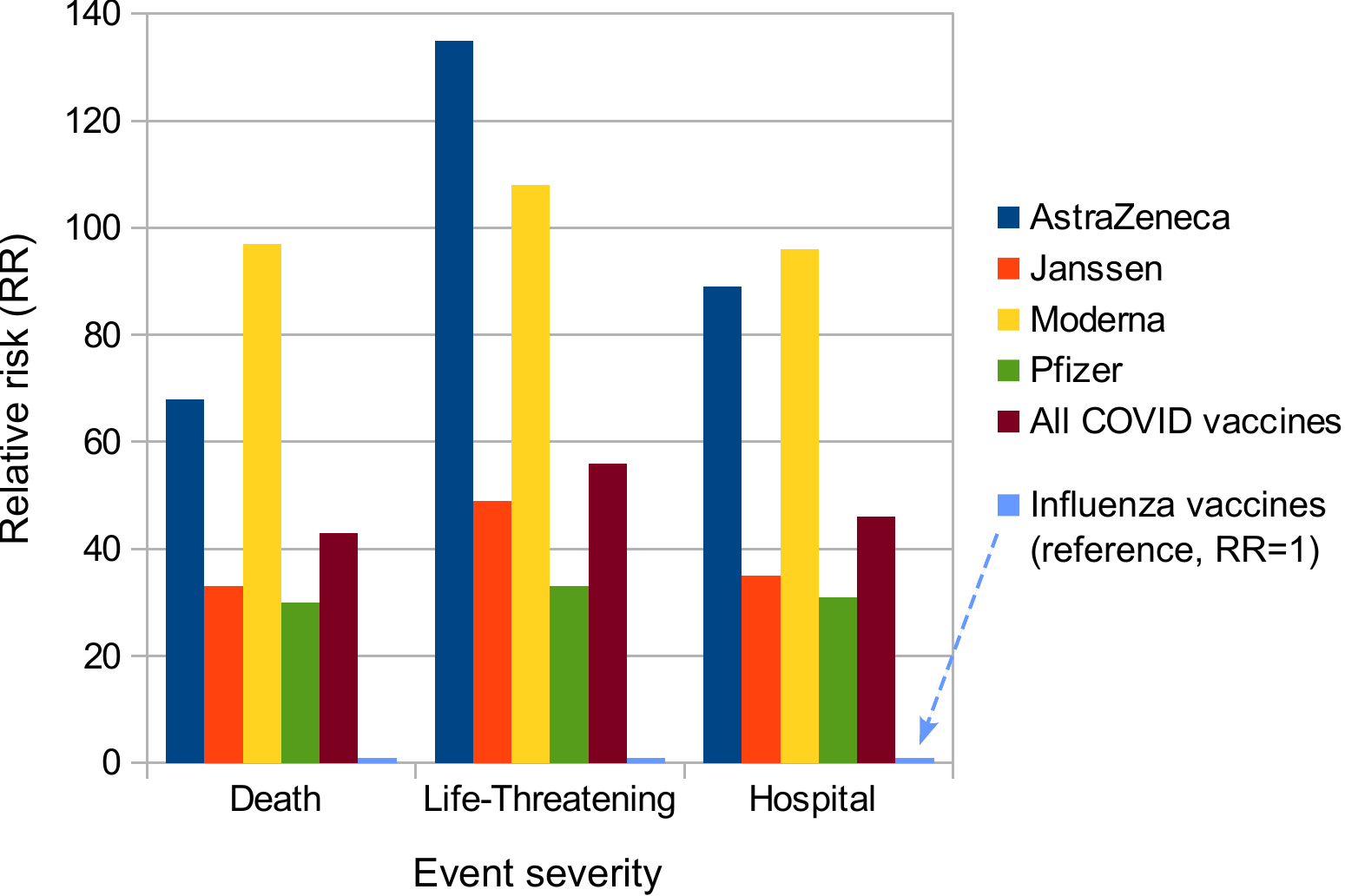
Montano [1] has addressed this question by comparing the four major COVID-19 vaccines to all influenza vaccines used within the EU and the US, using data from both the American vaccine adverse events reporting system (VAERS) and the EU’s very own EudraVigilance database. For the latter, his findings are summarized in Figure 1, which gives the risks of death, life-threatening reactions, and hospital admission associated being reported after each dose of a COVID vaccine, relative to the average of all influenza vaccines. Evidently, the risk is tens of times higher with each of the COVID-19 vaccines, across all three degrees of event severity. According to VAERS, the risk is even hundreds of times higher—it would literally be off the charts in this figure.
Montano’s data were published in early 2022. EMA’s own experts, and Ms. Kyriakides herself, should of course have already been on top of this highly concerning development, rather than waiting for an academic researcher to point it out to them. Their continued pretence that all is well even after this analysis had been put on the record is entirely indefensible.
2.2. Passive adverse event reporting systems are prone to under-reporting
In her reply, Ms. Kyriakides contrasts the number of 11,977 reported fatalities with that of 768 million administered doses. This comparison might suggest that the absolute risk of death after a COVID-19 injection is indeed low, regardless of the relative risk compared to other, conventional vaccines.
We should first note that the total stated by Ms. Kyriakides is suspicious. Independent researcher Brian Shilhavy, who has closely monitored both VAERS and Eurdavigilance, retrieved 46,999 reports of fatal cases from the latter system as of August 2022 [2]. With VAERS, similar discrepancies emerge between the numbers stated by officials and by independent analysts [3].
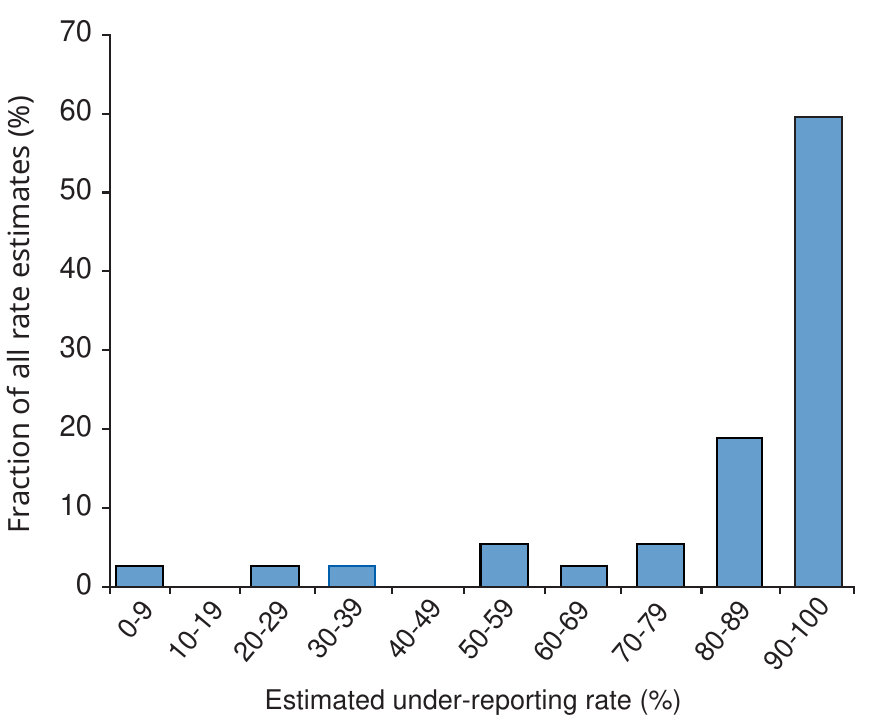
More fundamentally, however, we must observe that both VAERS and EudraVigilance are passive systems, i.e. they merely collect reports filed by healthcare practitioners or patients on their own initiative. It is generally understood that such systems are subject to significant under-reporting. A review on the subject, which surveyed 37 original studies, found that in most of these more than 90% of all adverse drug reactions went unreported (see Figure 2). Lazarus et al. [4], who looked at VAERS specifically, concluded that less than 1% of vaccine adverse events that occur end up being reported to this system. This estimate was made already in 2010, but we can see no reason to believe that the situation has substantially improved with respect to the COVID-19 vaccines.
2.3. Evidence of under-reporting of COVID-19 vaccine adverse events in EudraVigilance
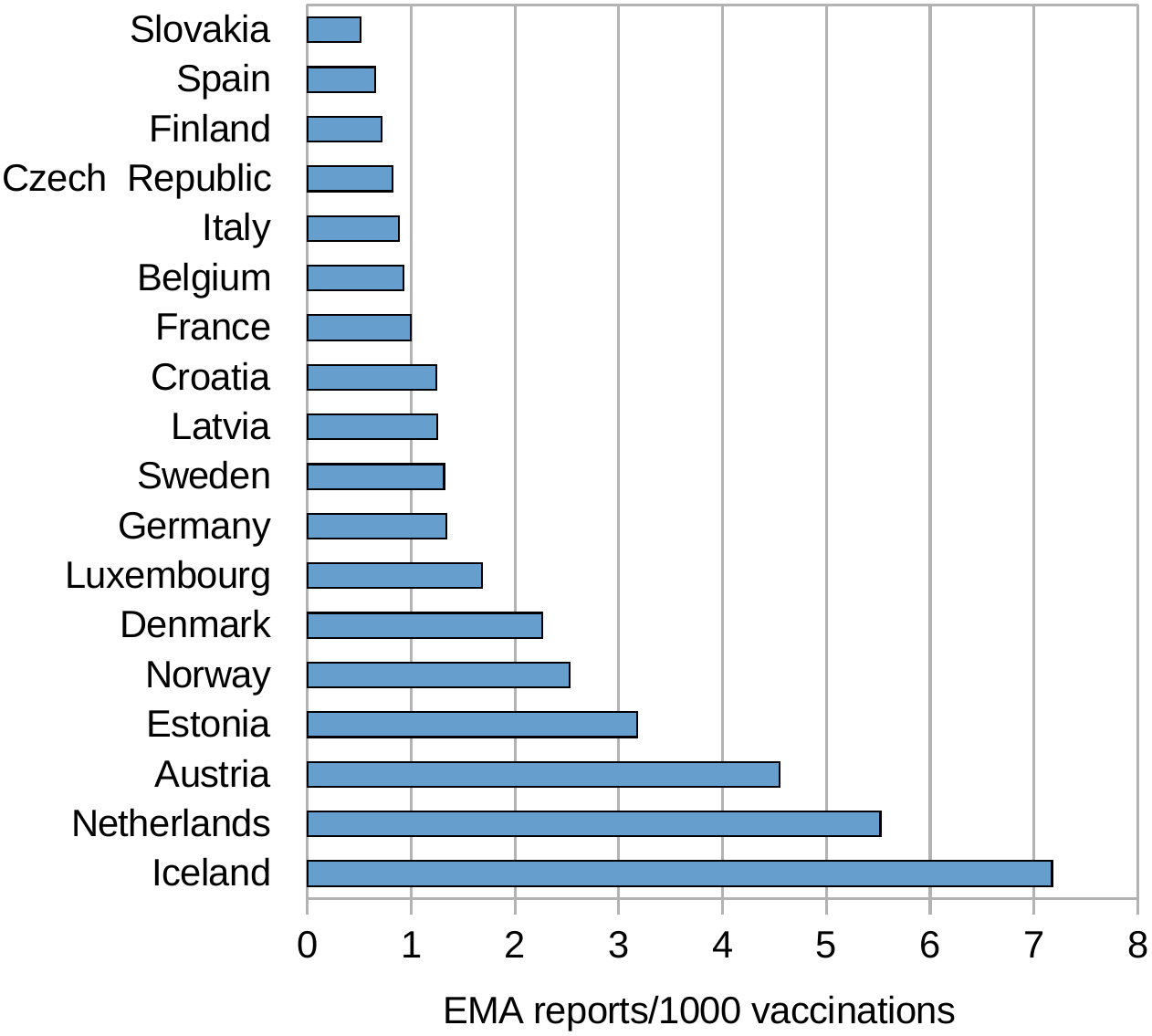
For EudraVigilance, we can derive clear indications of significant under-reporting by simply comparing the reporting rates between the system’s member countries. This has been done in Figure 3. The highest ratio of adverse event reports per 1000 vaccine injections is shown for Iceland. However, in this case the vaccination count extends only to the end of March 2022, while the number of adverse events was counted on September 9, which will of course inflate their incidence. Similar caveats apply to Slovakia and Latvia. But no such distortion exists with the Netherlands, where the two dates differ by only one week. We can therefore use the Dutch reporting rate as a reference.
In Spain, the reporting rate is only one eighth of the Dutch. Therefore, even if we very optimistically assumed that in Holland every single adverse event is reported, then we still would have to conclude that only one in eight adverse events gets reported in Spain. Also note the rather low reporting rates in the most populous EU countries—aside from Spain, these are Germany, France, and Italy. Overall, the reporting rate from all listed countries, weighted for population and excluding the Netherlands, is 21% of the Dutch reporting rate. Even though this figure most likely still overestimates the true reporting rate, it indicates that the problem of under-reporting remains significant and serious.
2.4. Estimates of COVID-19 vaccine fatalities from a representative survey in the United States
The above conclusions align with those arrived at by economist Mark Skidmore, based on a representative survey of COVID-19 vaccine decisions and experiences in the United States [8]. From his analysis of these data, Skidmore infers that approximately 278,000 vaccine-related fatalities had occurred already by the end of 2021, and within the United States alone. If a similar survey were conducted now, this number would likely be considerably higher. There is no reason to believe that the situation looks any rosier within the European Union.
2.5. Spikes in all-cause mortality correlate with COVID-19 vaccination
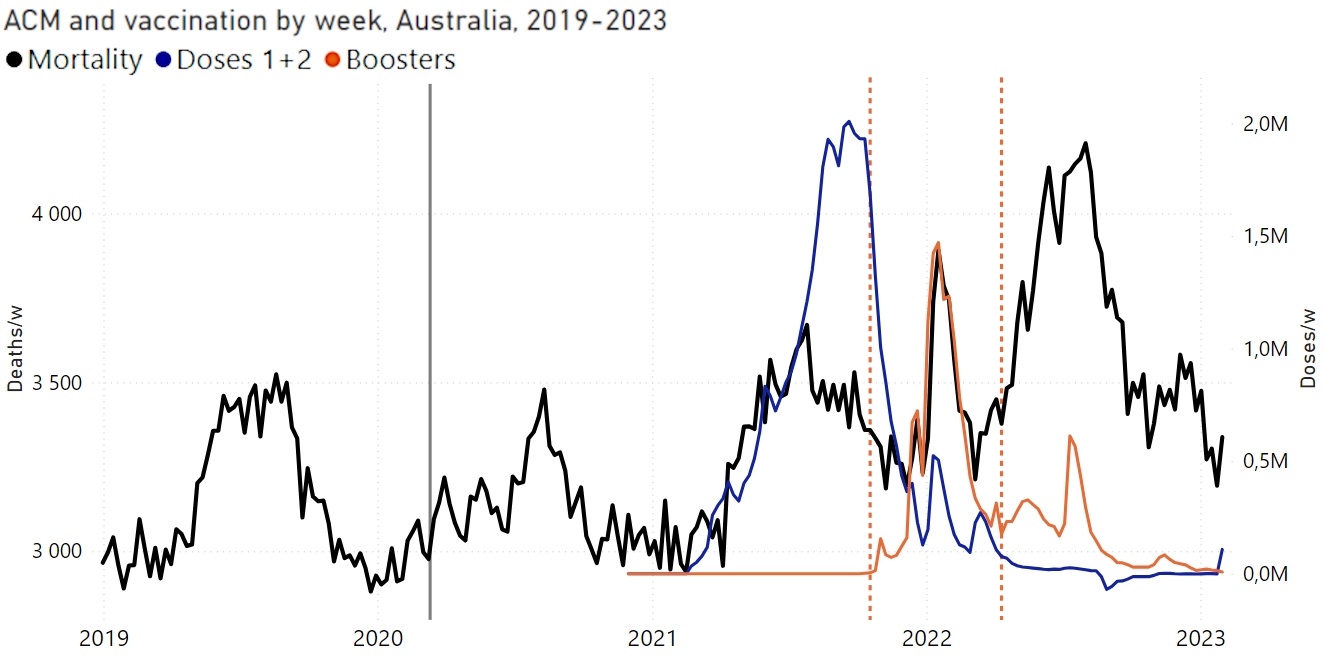
Multiple independent investigators have examined the relationship between trends in all-cause mortality and the roll-out of COVID-19 vaccines. They find a striking correlation of spikes in mortality with the timing of vaccination campaigns [9,10]. Furthermore, a clear correlation can be detected between national trends in mortality and rates of vaccine uptake [11]. As but one example, Figure 4 shows how each spike in vaccine injections coincides with one in all-cause mortality; and from the relative magnitude of those coinciding peaks, it appears that each successive dose is more effective in this regard. Also note that in 2020 mortality did not exceed that in 2019—obviously, the virus itself was not particularly deadly. This was of course already known before the vaccinations started, and it had been properly and formally published by leading epidemiologist John Ioannidis already in 2020, in the Bulletin of the WHO [12]. Such findings make it clear that the alleged “emergency,” which was invoked by the authorities to justify the extraordinary risky vaccination program, never existed.
2.6. On the proper use of passive adverse event reporting systems
Hazell and Shakir [5] draw the obvious and appropriate conclusions from the widespread and significant under-reporting bias of passive reporting systems, explaining what such systems can or cannot be used for:
In other words, EudraVigilance and similar institutions simply serve as early warning systems. While it must be understood that the magnitude of any signal from such a system will likely be underestimated, it can nevertheless be expected to highlight emerging problems quickly. Of course, this is exactly what occurred with the COVID-19 vaccines. EMA and the EU Commission, as the stewards of the EudraVigilance system, must therefore answer the following question: what did they do in response to this early and glaringly obvious danger signal? The only answer one can find on the public record is this: they did their best to bury it.
3. Is there really no proof of a causal connection to death and disease?
Ms. Kyriakides asserts that “only in very exceptional cases, deaths have been reported to be caused by the vaccine.” She cites a single relevant study and suggests that the problem affects only or mostly the adenoviral vaccines, and that the public is already being appropriately informed and cautioned.
In fact, and in contrast to the impression conveyed by Ms. Kyriakides, the number of published reports on fatal cases is substantial, in spite of widespread censorship.1 Ms. Kyriakides may find it instructive to peruse references [18–40], most of which attribute the death of one or more patients directly to vaccination, although some of the reports pertain to the deaths by COVID-19 of vaccinated patients, thus highlighting the futility of this “safe and effective” intervention. And as with the passive monitoring systems discussed above, we must assume that the number of published cases is only the tip of the iceberg. This is well illustrated by the work of Arne Burkhardt and Walter Lang, two emeritus professors of pathology, who have examined the autopsy materials of numerous patients that had died soon after receiving a COVID-19 vaccine. As stated in our previous summary of their work [41],2 these cases had initially been autopsied by other physicians, who had certified the cause of death as “natural” or “unknown.” Burkhardt and Lang became involved only because the bereaved families doubted these verdicts and sought a second opinion. It is remarkable, therefore, that Burkhardt and Lang found not just a few but the majority of these deaths to have been due to vaccination, with a high or even very high degree of probability.
We also must remind Ms. Kyriakides that the EMA, and by extension the EU Commission, were warned early on about the dangers of the gene-based COVID-19 vaccinations. In an urgent open letter to the EMA [43], a large number of physicians and medical scientists (also including the authors of this document) spelled out the risks and the likely key mechanism of acute vascular disease, many cases of which were already being reported very shortly after the vaccines had been approved for emergency use. This damage mechanism has since been fully substantiated by the histopathological studies carried out by Burkhardt, Lang, and others; and it has been found to affect not only the blood vessels but also organ-specific cells and tissues everywhere in the body. In one particularly important study, pathologist Michael Mörz has provided definitive evidence of a direct link between vaccine injection and destructive inflammation of the brain and the heart [44]. The patient in question, having experienced progressive deterioration after each injection, finally succumbed to the third one.
4. Conclusion
The evidence of harm and death due to the COVID-19 vaccines, which emerged within mere days of their roll-out, has since become utterly obvious and devastating. EMA’s failure to “detect a safety signal” constitutes a safety signal all unto itself. This signal has been detected by the public, which is turning its back on the vaccines and, by extension, on Ms. Kyriakides and Europe’s entire criminally negligent administration.
The toxicity of the gene-based vaccines was understood and predicted even before they were introduced, and the anticipated central mechanism of such toxicity has since been abundantly confirmed. This is discussed in more detail in our recent book “mRNA Vaccine Toxicity” [45], which can be downloaded and read for free. The book spells out that the grave harm observed with the COVID-19 vaccines must be expected with future gene-based vaccines against other infectious diseases also. We hope that you will spread this message and share it with your friends and family.
Notes
- Multiple studies that highlighted risks and dangers of COVID-19 vaccination were “retracted” after initial acceptance and publication [13–17], without any substantial or comprehensible justification. The number of studies which never even saw the light of day to begin with is very likely much higher.(go back)
- Prof. Burkhardt, though not a co-author, reviewed and approved our account of his work. He had co-authored a memorandum with Prof. Bhakdi at an earlier time, which pertained to a smaller number of patients but arrived at essentially the same conclusions [42]. Prof. Burkhardt died in 2023.(go back)
References
- (2022) Frequency and Associations of Adverse Reactions of COVID-19 Vaccines Reported to Pharmacovigilance Systems in the European Union and the United States. Frontiers in public health 9:756633
- (2022) 76,789 Deaths 6,089,773 Injuries Reported in U.S. and European Databases Following COVID-19 Vaccines.
- (2021) OpenVAERS.
- (2010) Electronic Support for Public Health—Vaccine Adverse Event Reporting System.
- (2006) Under-reporting of adverse drug reactions: a systematic review. Drug Saf. 29:385-96
- (2022) Coronavirus (COVID-19) Vaccinations.
- (2022) Tagesreport schwerwiegender Nebenwirkungen der Covid-19-Impfungen [Daily report on severe side effects of the COVID-19 vaccines].
- (2023) COVID-19 Illness and Vaccination Experiences in Social Circles Affect COVID-19 Vaccination Decisions. Sci. Publ. Health Pol. Law 4:208-226
- (2023) Age-stratified COVID-19 vaccine-dose fatality rate for Israel and Australia.
- (2023) COVID-19 vaccine-associated mortality in the Southern Hemisphere.
- (2021) Worldwide Bayesian Causal Impact Analysis of Vaccine Administration on Deaths and Cases Associated with COVID-19: A Big Data Analysis of145 Countries. ResearchGate DOI:10.13140/RG.2.2.34214.65605
- (2020) Infection fatality rate of COVID-19 inferred from seroprevalence data. Bull. World Health Organ. p. BLT.20.265892
- (2023) A Systematic Review of Autopsy Findings in Deaths after COVID-19 Vaccination.
- (2021) SARS-CoV-2 Spike Impairs DNA Damage Repair and Inhibits V(D)J Recombination In Vitro. Viruses 13:2056
- (2021) Why are we vaccinating children against COVID-19?. Toxicol. Rep. 8:1665-1684
- (2021) A Report on Myocarditis Adverse Events in the U.S. Vaccine Adverse Events Reporting System (VAERS) in Association with COVID-19 Injectable Biological Products. Current problems in cardiology p. 101011
- (2023) RETRACTED ARTICLE: The role of social circle COVID-19 illness and vaccination experiences in COVID-19 vaccination decisions: an online survey of the United States population. BMC Infect. Dis. 23:51
- (2021) Fatal Case of Rhabdomyolysis Post-COVID-19 Vaccine. Infect. Drug Resist. 14:3929-3935
- (2021) Cerebral Venous Sinus Thrombosis With Severe Thrombocytopenia: A Fatal Adverse Event After Johnson & Johnson COVID-19 Vaccination. Neurol. Clin. Pract. 11:e971-e974
- (2022) First Identified Case of Fatal Fulminant Necrotizing Eosinophilic Myocarditis Following the Initial Dose of the Pfizer-BioNTech mRNA COVID-19 Vaccine (BNT162b2, Comirnaty): an Extremely Rare Idiosyncratic Hypersensitivity Reaction. J. Clin. Immunol. DOI:10.1007/s10875-021-01187-0
- (2022) Fatal Outcome of COVID-19 Relapse in a Fully Vaccinated Patient with Non-Hodgkin Lymphoma Receiving Maintenance Therapy with the Anti-CD20 Monoclonal Antibody Obinutuzumab: A Case Report. Vaccines 10
- (2021) Myocarditis-induced Sudden Death after BNT162b2 mRNA COVID-19 Vaccination in Korea: Case Report Focusing on Histopathological Findings. J. Korean Med. Sci. 36:e286
- (2021) Intracerebral Hemorrhage due to Thrombosis with Thrombocytopenia Syndrome after Vaccination against COVID-19: the First Fatal Case in Korea. J. Korean Med. Sci. 36:e223
- (2023) Death from COVID-19 in a Fully Vaccinated Subject: A Complete Autopsy Report. Vaccines 11
- (2021) Fatal Multisystem Inflammatory Syndrome in Adult after SARS-CoV-2 Natural Infection and COVID-19 Vaccination. Emerg. Infect. Dis. 27:2914-2918
- (2022) High viral loads: what drives fatal cases of COVID-19 in vaccinees? An autopsy study. Mod. Pathol. DOI:10.1038/s41379-022-01069-9
- (2023) Sudden Death Associated With Possible Flare-Ups of Multiple Sclerosis After COVID-19 Vaccination and Infection: A Case Report and Literature Review. J. Korean Med. Sci. 38:e78
- (2022) Fatal Acute Hemorrhagic Encephalomyelitis and Antiphospholipid Antibodies following SARS-CoV-2 Vaccination: A Case Report. Vaccines 10
- (2022) First Identified Case of Fatal Fulminant Eosinophilic Myocarditis Following the Initial Dose of the Pfizer-BioNTech mRNA COVID-19 Vaccine (BNT162b2, Comirnaty): an Extremely Rare Idiosyncratic Necrotizing Hypersensitivity Reaction Different to Hypersensitivity or Drug-Induced Myocarditis. J. Clin. Immunol. 42:736-737
- (2023) Lessons Learnt from Case Series of Out-of-hospital Cardiac Arrest and Unexpected Death after COVID-19 Vaccination. Intern. Med. DOI:10.2169/internalmedicine.2298-23
- (2022) Acute transverse myelitis after BNT162b2 vaccination against COVID-19: Report of a fatal case and review of the literature. J. Neurol. Sci. 434:120102
- (2022) Fatal Acute Disseminated Encephalomyelitis Post-COVID-19 Vaccination: A Rare Case Report. Cureus 14:e31810
- (2023) A case of fatal multi-organ inflammation following COVID-19 vaccination. Leg. Med. Tokyo 63:102244
- (2022) A Three-Case Series of Thrombotic Deaths in Patients over 50 with Comorbidities Temporally after modRNA COVID-19 Vaccination. Pathogens 11
- (2021) Postmortem investigation of fatalities following vaccination with COVID-19 vaccines. Int. J. Legal Med. 135:2335-2345
- (2022) First and fatal case of autoimmune acquired factor XIII/13 deficiency after COVID-19/SARS-CoV-2 vaccination. Am. J. Hematol. 97:243-245
- (2022) An Interesting Case of Fatal Myasthenic Crisis Probably Induced by the COVID-19 Vaccine. Cureus 14:e23251
- (2022) Fatal Cerebral Venous Thrombosis in a Pregnant Woman with Inherited Antithrombin Deficiency after BNT162b2 mRNA COVID-19 Vaccination. Tohoku J. Exp. Med. 258:327-332
- (2022) Brain death in a vaccinated patient with COVID-19 infection. Clin Imaging 81:92-95
- (2022) TAFRO syndrome with a fatal clinical course following BNT162b2 mRNA (Pfizer-BioNTech) COVID-19 vaccination: A case report. J. Infect. Chemother. 28:1008-1011
- (2022) Vascular and organ damage induced by mRNA vaccines: irrefutable proof of causality.
- (2021) On COVID vaccines: why they cannot work, and irrefutable evidence of their causative role in deaths after vaccination.
- (2021) Urgent Open Letter from Doctors and Scientists to the European Medicines Agency regarding COVID-19 Vaccine Safety Concerns.
- (2022) A Case Report: Multifocal Necrotizing Encephalitis and Myocarditis after BNT162b2 mRNA Vaccination against Covid-19. Vaccines 10:2022060308
- (2023) mRNA Vaccine Toxicity.