Michael Palmer, MD
One of the main themes in my book Hiroshima Revisited is the use of mustard gas to cause “radiation sickness” among the victims of the faked “atomic” bombings. In this post, I am going to give an overview of that evidence, enriched with some pertinent eyewitness testimony not quoted in the book.
1. On mustard gas
Mustard gas, or sulfur mustard was first used during World War 1. Even though introduced only in 1917, it caused more casualties than any of the previously used battle gases. A key reason for this high lethality is that it bypasses the protection afforded by gas masks by attacking the skin, which it causes to blister, and is also taken up quite effectively across the skin. In those not protected by gas masks, it causes severe lung damage; this was reported in Iranian soldiers exposed to mustard gas used by Iraq in the war between the two countries [1].
Aside from causing acute damage to the skin and the lungs, mustard gas mimics the destructive effects of radiation on rapidly proliferating tissues such as the bone marrow, the hair follicles, and the intestinal mucous membranes. This similarity was recognized clinically as early as 1919 [2–4]. With both radiation and mustard gas, the underlying mechanism is now understood to be DNA damage.
The U.S. military had stockpiled mustard gas during World War 2 and also filled it into aerial bombs [5]. Thus, it would have been prepared for its use in the bombings of both cities.
2. Testimony which supports the use of mustard gas in the “atomic” bombings
Eyewitness reports which suggest the use of mustard gas are not in short supply. The possibility that some kind of poison gas had been released at Hiroshima was brought up early on by Dr. Masao Tsuzuki, the leading Japanese member on the U.S.-Japanese “Joint Commission” of medical scientists convened to investigate the aftermath of the bombing. The historian Sey Nishimura [6] quotes from a 1945 article by Tsuzuki:
The first Western journalist to report from Hiroshima, the Australian Wilfred Burchett [7],1 also brings up poison gas:
According to Burchett, the Japanese he spoke to believed that the smell
and he reports that the Japanese then engaged in clearing the debris from the city centre were wearing gauze masks over their faces to protect themselves from the gas.
Among 105 witnesses who experienced the Hiroshima bombing as school age children, and whose memories were collected and published by the Japanese teacher Arata [8], 13 explicitly mention poisonous gas or fumes. One of them, Hisato Itoh, died of leukaemia shortly after writing his account, which contains this statement:
Here are some more quotes by several other schoolchildren:
Satomi Kanekuni: On August 6 when the bomb fell, Father and Mother were living in Yanagi-machi. They were trapped by the house when it fell down and inhaled poisonous gas.
Junya Kojima: When I was five years old, there was the atom bomb explosion. My father was at his office then. I guess he breathed in poison gas … he soon died.
Yohko Kuwabara: Just then, I was blinded for a moment by piercing flash of bright light, and the air filled with yellow smoke like poison gas.
Yoshiaki Wada: My mother … breathed the poison gas from the atom bomb. That’s why she was so bad.
While not all of these reports point to mustard gas specifically, the respiratory symptoms and the hair loss mentioned in some of them are both quite suggestive. So is the sulfuric smell reported by Burchett in early September—both the smell itself and its long persistence point to mustard gas.
It also is rather striking how most of these witnesses draw a straight line from the atom bomb to the poisonous gas; it appears that they have been led to believe that atomic bombs somehow give rise to poisonous gas, which is of course untrue. The same error even found its way into the medical literature [9, p. 464]:
3. How can we decide between radiation and mustard gas effects in Hiroshima?
There are two kinds of evidence that we can use here:
- effects of nuclear radiation that should have been observed but were not, and
- effects of mustard gas that were observed but should not have been.
In the first category, there are multiple reports of miraculous survival among those who should have died, because they had been exposed to “theoretically exposed to lethal doses of radiation” [10]. This is discussed in some detail in the book. In the remainder of this article, we will focus on the second category—namely, observations in bombing victims which directly point to the use of mustard gas.
4. Acute lung damage and respiratory distress
While mustard gas has radiation-like effects on the bone marrow, the hair follicles, and other sensitive tissues, there nevertheless are telling differences between the two. Inhalation of mustard gas will cause acute and severe lung damage. In contrast, in those exposed to rapidly fatal radiation doses, it is the brain, not the lung, which shuts down first [11, p. 218]:
In contrast, many early victims at Hiroshima and Nagasaki suffered the most intense respiratory distress. An eyewitness from Hiroshima, Mr. Hashimoto, recounts from the day of the bombing [12]:
Mr. Hashimoto also describes the aftermath:
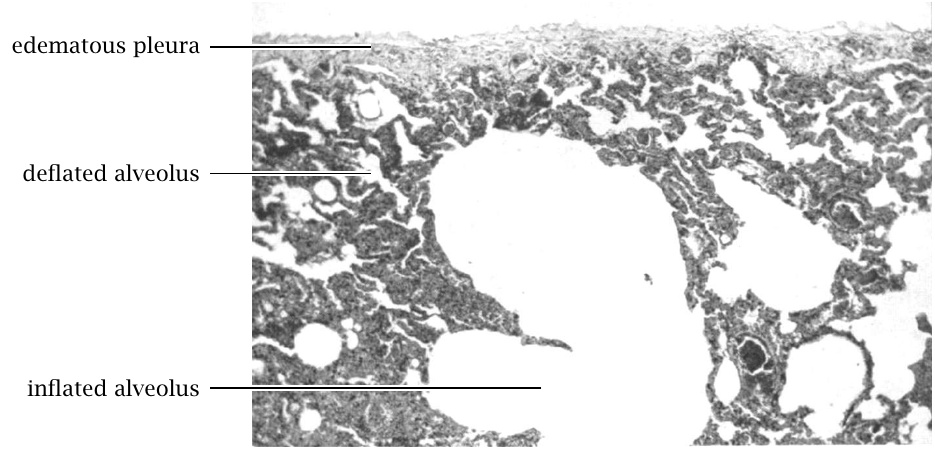
The “oozing froth” noted by the astute Mr. Hashimoto is an indication of toxic lung edema, which is also known from cases of unprotected exposure to mustard gas [1]. Other effects seen in early fatalities are lung emphysema, i.e. excessively inflated lung tissue, together with atelectasis, i.e. compressed or deflated lung tissue (see Figure 2). The simultaneous presence of emphysema and atelectasis is also described in standard works on mustard gas poisonings that were published after World War I [4,13].
5. Acute radiation sickness in people who weren’t near the alleged nuclear bomb
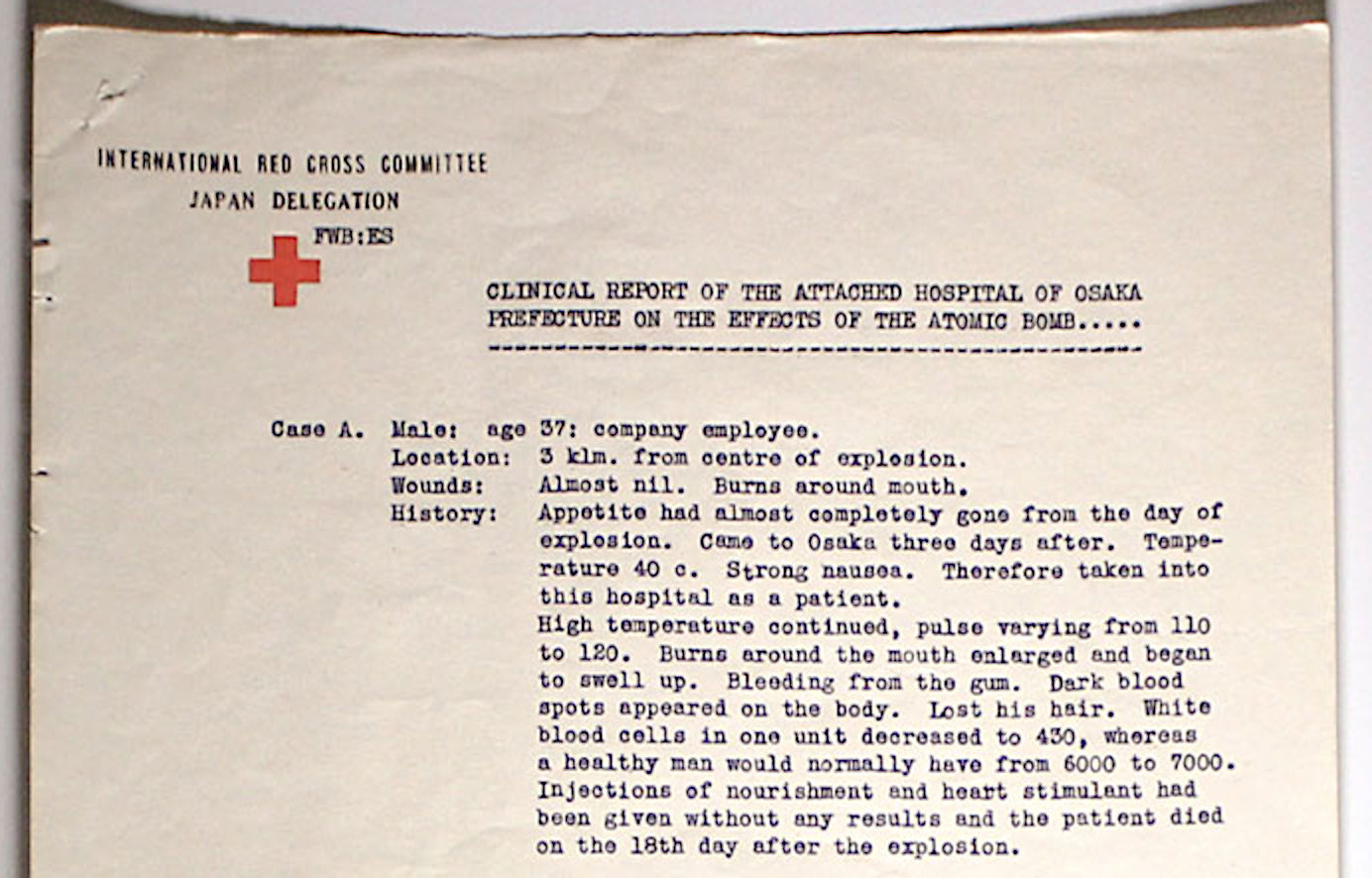
According to the official story of the bombings, rapidly fatal radiation doses could only have been received 1) within less than 1.5 km from the center of the detonation, and 2) at the exact time of the detonation [15]. However, there have been numerous cases of “radiation sickness” in persons who were not near the bombing when it happened, but who entered the zone of destruction shortly afterwards. An early case report is shown in Figure 3. The available statistical evidence on such cases is presented in Chapter 8 of my book [16].
Anecdotal evidence further reinforces this point. For example, here is an excerpt from the recollections of Toyofumi Ogura, a history professor from Hiroshima University [18]:
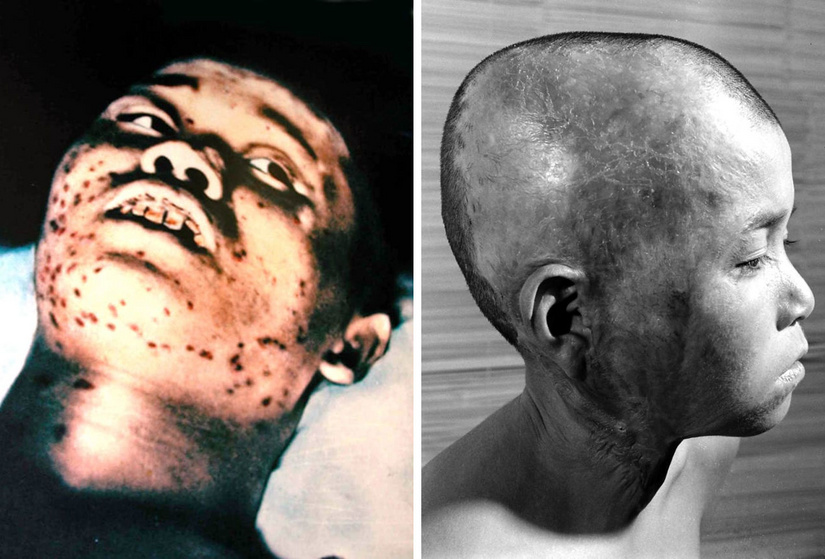
6. Skin lesions
Mustard gas is a blistering agent—it disrupts the connection between the skin and the underlying tissues. Skin blisters are quite commonly described in witness testimony. Ogura’s daughter describes the aspect of her mother’s body after her death due to “radiation sickness”:
Even skin which has not yet detached from its support may do so when subjected to shear stress. Here is a description by Col. Stewart F. Alexander, the US military physician who had looked after the victims of a Luftwaffe attack on an American freight ship which had been carrying mustard gas, in the Italian port city of Bari [19]:
And here, for comparison, one more quote from Ogura’s book. As he makes his way across the city in search of his relatives, on the day of the bombing, he comes upon an obstacle:
Since the dead woman’s knees were raised slightly, I grasped the ankles to move the legs aside slightly so that I could pass without having to step over the body. But as I tried to lift the legs, I thought I felt my hands slip. It was an indescribably weird sensation. Looking down at my hands, I saw the exposed muscles of both legs, from the knees down, glinting in the sun. … The skin had peeled off and had gathered at the ankles, all wrinkled up.
I crouched there for a minute, with the shock of it.
Even though pathology reports on victims from Hiroshima are scarce, those that one can find also contain descriptions of peeling skin.
7. Conclusion
So there you have it—the clinical signs one finds described by eyewitnesses and by pathologists clearly indicate that the malodorous “atom-bomb gas” that was perceived by many during and after the bombings was none other than mustard gas. This was, however, not the only deadly weapon deployed in these bombings; another one was napalm. This will be discussed in a separate post.
Notes
- This report first appeared under the name ‘Peter Burchett’ in the Daily Express on September fifth, 1945.
References
- (1991) The role of bronchoscopy in pulmonary complications due to mustard gas inhalation. Chest 100:1436-41
- (1919) The Blood and Bone Marrow in Yellow Cross Gas (Mustard Gas) Poisoning: Changes produced in the Bone Marrow of Fatal Cases. J. Med. Res. 40:497-508.3
- (1920) The Effects Of Intravenous Injections Of Dichloroethylsulfide In Rabbits, With Special Reference To Its Leucotoxic Action. J. Exp. Med. 31:71-94
- (1919) The medical aspects of mustard gas poisoning (Mosby).
- (1947) U.S. Explosive Ordnance (U.S. Navy Bureau of Ordnance).
- (1995) Censorship of the atomic bomb casualty reports in occupied Japan. A complete ban vs temporary delay. JAMA 274:520-2
- (2007) The atomic plague in: Rebel journalism: the writings of Wilfred Burchett.
- (1980) Children of Hiroshima (Publishing Committee for “Children of Hiroshima”).
- (1974) Cancer and leukemia developing among atomic bomb survivors in: Handbuch der allgemeinen Pathology [Handbook of general pathology] (Springer).
- (1956) Medical effects of the atomic bomb in Japan (McGraw-Hill).
- (2019) Radiobiology for the Radiologist (Wolters Kluwer Health).
- (1955) Hiroshima Diary: The Journal of a Japanese Physician, August 6-September 30, 1945 (University of North Carolina Press).
- (1933) The residual effects of warfare gases.
- (1949) Pathology of atomic bomb casualties. Am. J. Pathol. 25:853-1027
- (2006) Dose estimation for atomic bomb survivor studies: its evolution and present status. Radiat. Res. 166:219-54
- (2020) Hiroshima revisited: the evidence that napalm and mustard gas helped fake the atomic bombings.
- (2015) ICRC report on the effects of the atomic bomb at Hiroshima. International Review of the Red Cross 97:859-882
- (1997) Letters from the end of the world (Kodansha International).
- (1947) Medical report on the Bari Harbor mustard casualties. Mil. Surg. 101:1-17